





Empirical Evaluation of Inter-Hemispheric Training; Part II
by Siegfried Othmer | October 27th, 2005Last week we presented data on the impulsivity subtest of the TOVA CPT for clients who received neurofeedback training exclusively with the inter-hemispheric placements. This week we present companion data on the inattention subtest. The data were compiled for us by John Putman, and were recently published in the Journal of Neurotherapy (Volume 9 (1), pp 37-52). Complementary data are also shown where the inter-hemispheric training predominated, but where lateralized placements were also used. Comparison of results is then made to data analyzed for us years ago by David Kaiser, data that refer to the lateralized training that was done at that time. By folding the lateralized placements in with the inter-hemispheric we are essentially comparing the best we are capable of doing now with the best we were capable of doing earlier. An improvement in results is indicated for the current methods.
Last week we made the case for impulsivity as the best possible index of that we can derive from CPTs for our purposes. We argued that impulsivity indexed the very disregulation that we address with neurofeedback. Nevertheless, we should also look at inattention. In this measure we may be dealing with “organicity” that cannot be remedied with neurofeedback, regardless of methodology, and we have no independent assessment of this available. The issue of organicity must remain a confound in our comparisons.
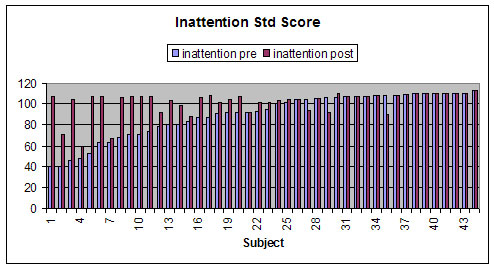
In Figure 1 we show the inattention group data that appeared in the recent publication. Two features are particularly noteworthy. First of all, observe the ceiling effect at the nominal standard score of 108. This is the value somewhat arbitrarily assigned by the developers of the TOVA for the case of zero omission errors. No one can score better on this subtest, so the normal curve is in fact truncated, looking very much like Half Dome. The second observation is that the part of the distribution that scored above norms tended to maintain their score.
In Figure 2, we show the larger data set that also includes cases where some lateralized training was done along with the inter-hemispheric placements. Both sets of data refer to nominally twenty-session retest data, and hence do not represent the final end-point of training in most of these cases. This is done simply because the CPT normalization tends to occur early in training, particularly in the case of inattention (if it is going to occur at all). This also facilitates comparison with earlier data, which also refer to 20-session retests.

In Figure 3 we show early group data that were compiled by David Kaiser on our prior lateralized trainings (“C3beta” plus “C4 SMR”). These data refer to work done some ten years ago. The data are rank-ordered by level of initial deficit, grouped into bins in terms of standard score. Significantly, the group in greatest deficit, at least four standard deviations below norms, collectively shows progress by two standard deviations. (In this plot, those who scored more than four standard deviations below norms were assigned a standard score of forty. This is because the performance curve is unlikely to be Gaussian beyond four standard deviations. The numbers can get very large, and if that were allowed to enter the calculation, then it would be these extreme cases that would dominate. (For example, a single case could improve by a hundred points or more in standard score and skew the whole data set for that bin.) We analyzed the data in the same way years ago.

In Figure 4 we show a comparison of the latest data with the historical data. In all but the most severe category, the modern results appear nominally better. We have previously argued that a statistical comparison cannot be justified here because the populations are not at all comparable. If that difference is factored in, then the modern data look even better. The comparison looks worse in the case of those in most severe deficit. But then these are the very ones where organicity is most likely an issue. So we are victimized by statistics here. The earlier data sample was much larger (>350) than the more recent one (107), so the modern data are more subject to population variance. Additionally, the fact that we are working with a much more severely impaired population in recent times may be manifested here.

In summary, then, we see the inattention data largely confirming the conclusion we had already formed on the basis of the impulsivity data, namely that modern methods are superior, and allow our methodology to be applied to a more severely impacted population.
Next week we will look at some individual cases where one might ask whether the training reduced the level of functioning. One of the concerns about inter-hemispheric training has been that in some cases it might lead to adverse outcomes. This concern follows from the use of reinforcement frequencies even in the range of theta and delta bands. Of course we are now allowing the addition of lateralized trainings if that turns out to be an advantage, i.e. if the burden cannot be borne entirely by the inter-hemispheric training. Given that admixture, will we still be able to exonerate the inter-hemispheric training entirely, provided the data were to support that judgment? The answer is yes. When lateralized training is added to the mix, it is not the SMR/beta training of old. Rather, it involves training in the same frequency range as the inter-hemispheric. So if someone is inclined to raise their eyebrows about a reinforcement paradigm at 4-7 Hz inter-hemispherically, then they cannot at the same time be sanguine about lateralized trainings in the same frequency range.
Subsequently, we will look at some modeling to show why the bipolar placements in general, and the inter-hemispheric ones in particular, should have such universally beneficial effects.