





Neurofeedback in the Biofeedback Perspective
by Siegfried Othmer | October 2nd, 2017
Over the years, we have gone to great lengths to argue that neurofeedback is merely biofeedback by other means, and if anything, ILF (Infra-Low Frequency) neurofeedback is even more analogous to traditional biofeedback than standard EEG training. It works with slowly varying physiological signals, and is oriented toward the most basic regulatory functions, including autonomic regulation and arousal regulation. ILF training has clinical priorities in common with somatic biofeedback. The EEG plays only a secondary role in the actual training, and none in the ILF component. Further, the slowly varying signal also involves significant non-neuronal components. A further commonality is that it does not involve operant conditioning.
Indeed, ILF neurofeedback appears more analogous to somatic biofeedback than it does to conventional neurofeedback. The topic of commonalities has been an important one to address. It serves as a gesture across the fissure that divides the field to this day, and as an attempt to promote its conceptual reunification. But the complementary truth, that ILF neurofeedback is distinctly different from somatic biofeedback in some crucial respects, must also be appreciated.
Standard somatic biofeedback involves the whole person in the process. The trainee watching the finger temperature gauge is reinforced in the training by virtue of the temperature rising, but it is rising because the trainee is actively supporting the process of shifting state toward lower sympathetic arousal by various strategies. The good biofeedback therapist is a coach who conveys various active strategies to be adopted. These might involve autogenic training, progressive relaxation, the learning of abdominal breathing, slowing the breath, thought-stopping, mindfulness or visualization strategies, etc. Alternatively, the rise might occur because of a more passive process. This might mean nothing more than shifting toward an internal focus and quieting the intrusive thoughts that agitate the mind, a mindfulness strategy. Even just attending to the biofeedback measure—via the exclusion of other distractions—may suffice. By contrast, the path to successful ILF neurofeedback does not depend on any active involvement on the part of the trainee.
This distinction was brought home to me forcefully years ago when I was using temperature training to warm my cold feet. The process worked charmingly, even though my only overt strategy was to focus single-mindedly on the project of raising the thermometer reading. I could raise the temperature five degrees or more within fifteen minutes. But the process was still quite slow—and very boring. Since the temperature gauge moved slowly, I thought I could get away with reading a journal article at the same time, just glancing at the thermometer occasionally, to see that things were still on track. As soon as I engaged with the technical material, however, my foot temperature dropped like a stone. A sympathetic shift was initiated, and my feet paid the price. This was not a failure of biofeedback, but rather a failure of execution on my part. I could not absent myself from the task of state management and yet sustain the upward progress. The biofeedback could not be done in “background,” so to speak, or in autopilot, or in subroutine—choose your metaphor. Though well-launched, the process was not self-sustaining.
This characteristic of biofeedback has been well recognized within the field, and is even reflected in the early terminology that was adopted to describe the procedure, namely “voluntary controls.” The essential breakthrough in those days was the recognition that the autonomic nervous system was not purely autonomic, but could in fact be usefully steered via volitional processes and thus trained toward healthier operating points (homeostasis). Taking volition out of the process is the equivalent of taking one’s foot off the accelerator. The process grinds to a halt.
The most dramatic proof of this proposition was John Basmajian’s work with the training of control over the firing of individual motor units (Ref.). Trainees were, in many instances, capable of training several motor units in real-time control of their firing events, and some could achieve that within 90 minutes. Here the voluntary control was quite explicit. Clearly, a control loop had been established that involved the trainee’s intentionality, on the one hand, and a single motor neuron, on the other.
In the early days of neurofeedback, this same model was extended to the EEG training of human subjects. As late as 2009, Lubar was still adamant on the issue that young children could not be usefully trained because they did not have the cognitive maturity to play their part in the process and further, that they were unlikely to retain their gains, if any were achieved (personal correspondence). Throughout our time in this field, however, we have also had opportunities to train very young children, including infants, even infants who were cognitively compromised due to a near-drowning incident.
There is no room for cognition and volition to play the same role here as in biofeedback. Frequency-based neurofeedback engages the brain directly, and thus does not depend upon engaging the person, at least not to the same degree. Very different rules may then apply. It is true that traditional neurofeedback is typically reinforcement-based, but often these reinforcements refer to brain events that do not rise to the level of conscious awareness. They are cues to the brain more than to the person. In the case of ILF neurofeedback, even such discrete reinforcements fall away. Therefore, ILF neurofeedback cannot be judged in the perspective of traditional biofeedback or even standard reinforcement-based neurofeedback.
A new term is coming into currency to describe this kind of process: closed-loop training. The term does not tell us anything new, however. Feedback always closes the loop. Implicit is that the closed loop involves the brain directly rather than the person who possesses the brain. And ILF training is perhaps the best example of this approach. The signal is slow and therefore boring. But the brain could hardly be more intrigued. It ‘gets it’ right away, and the trainee starts shifting state accordingly within mere minutes.
In truth, however, we have been doing non-volitional training all along. After all, we have been working successfully with infants since the beginning. Margaret Ayers had been doing so long before we came along in 1985. But what was necessarily true with infants was also true in more generality. It has always been the non-volitional aspect of the training that has borne the burden, irrespective of any cognitive involvement that we may have promoted along the way, and irrespective of any overt reinforcements we may have introduced.
It follows that if the training is non-volitional in nature, then it should also be doable in background. Not only is this possible, but this has become our standard approach. Most of our trainees prefer to watch videos while they train. They pay no attention at all to the feedback signal, and indeed may not even be aware of how the feedback is being encoded. Not only is cognitive involvement entirely superfluous here; we must allow for the possibility that it could even be counter-productive. There is yet another term for this kind of training: covert neurofeedback.
We can look at the last thirty years of development as a time of refinement. We went from crude, discrete reinforcements of various kinds to no explicit reinforcements at all. We went from placing ourselves entirely in charge of the process to finally allowing the brain to oversee its own affairs. That means the process has become a continuous one. It has become a matter of the brain engaging with the unfolding signal and reacting to it within the scope of its own mysterious schema.
This recognition became inescapable once discrete rewards were no longer at issue. In truth, it has been the case all along, as we always showed the brain the EEG dynamics in the training band along with the discrete rewards. Over the years, we came to realize that our own external steering of the process would always be somewhat crude and simplistic. At the same time, we were needlessly constraining the information flow to the brain. But in the end, it did not matter that much because the brain was all along having a different experience than we had intended for it. It was involved in the non-volitional aspect of the training, a fact that we were slow to appreciate.
Adoption of the response frequency optimization procedure was an early accommodation to the brain’s prerogatives. Once the question was asked, the brain readily furnished the answer—and it was not subtle. And now we realize that when the brain is offered the real-time information that it needs, the training process is both rapid, highly impactful, and refined. Brain self-regulation occurs at a level of such subtlety that it cannot be outsourced. The brain needs information; it is not in need of instruction —particularly not from people who know as little about brain function as we do.
In view of the above, it becomes apparent why academic researchers get such bum results with their neurofeedback studies. Typically, they will have gone to great lengths to emulate the overt reinforcement-based aspect of the training, at the expense of any “extraneous” component. In the pursuit of a pristine operant conditioning design, the training procedures have been impoverished. Unsurprisingly, the results are often either disappointing relative to objectives, or not much better than sham training.
It may be useful at this point to elucidate further the difference between the two kinds of training—traditional biofeedback and neurofeedback. One way to put it is that traditional biofeedback looks at consequences whereas EEG feedback engages more directly with causes. The temperature sensor in biofeedback registers that a shift in autonomic balance has occurred, whereas EEG neurofeedback or ILF training may bring such a shift about by engaging at the level of brain mechanisms.
The significance of the temperature measurement is registered in consciousness. The measurement is not of intrinsic significance to the brain. The EEG signal, or the ILF signal, on the other hand, has only a tenuous connection with matters of interest to the trainee or the clinician. Yet the signal is quickly recognized by the brain as being relevant to its own ongoing activities. The one represents an action item for the person; the other is an action item for the brain—and only for the brain. The signal holds no meaning for the person.
With neurofeedback, we have moved up the causal chain, closer to the source of the action. On the other hand, we are still dealing with consequences rather than causes. This is inescapable. We are not given the opportunity to get back to the ultimate causes, and that is not only because the causal chains are complex or obscure. The problem is inherent in the process of measurement. Once we’ve come to terms with that, it becomes easier to acknowledge that our primary task is to facilitate the brain’s engagement with the signal rather than our own.
It is apparent, then, that neurofeedback has become something very different from traditional biofeedback. Understanding the one does not confer understanding of the other. It remains true, however, that each has a distinct role to play in the promotion of self-regulatory competence. Dysregulation is not a unitary entity. It can be lodged in specific physiological systems and may have to be addressed with some specificity in the various systems.
This can be readily illustrated with a case we encountered just recently. While tracking someone through neurofeedback training with physiological measures, we observed that the trainee had good heart rate variability, decent heart rate, and good finger temperature (96 degrees!), and yet exhibited high blood pressure (for which the client was on medication). Did high blood pressure not indicate vasoconstriction? Why did that not register in finger temperature? The only clue to the hypertension was the blood pressure measurement itself. The profound dysregulation in that system did not register prominently elsewhere.
Recently, we’ve entertained the thought that the concept of sensory substitution—currently popularized by David Eagleman—may be a useful metaphor for neurofeedback that helps to sharpen the distinction. In the case of hand temperature training, we have direct, independent awareness of our hand temperature. We do not completely depend on the instrumentation. We have the historical event of Swami Rama’s demonstration of differential control of palm temperature to prove that instrumentation is not necessary for hand temperature training. Over the course of less than fifteen minutes, he was able to induce an eleven-degree temperature difference between two regions of his palm. (He allowed that it had been exceedingly challenging for him to develop that capability.)
Matters are different when it comes to the EEG or the Slow Cortical Potential. We lack internal awarenesss here, and we are therefore completely dependent upon the instrumentation to accomplish the training task. Matters are analogous to the situation in which a blind person has his visual field mapped to a tactile array placed on his tongue, for example, and the brain does the rest in terms of making sense of this novel signal stream. In this case, of course, there is a long learning curve at the outset. In the case of neurofeedback, there merely needs to be recognition of the signal to close the loop, and that can happen quite rapidly.
Since there is no necessary cognitive involvement, the process can even be a continuous one. Framed as a sensory substitution device, our neurofeedback system has become a kind of cerebral prosthesis in support of the brain’s ongoing self-regulatory burdens. All this is very far afield from the way we utilize somatic biofeedback.
None of this means, however, that the prospective role of traditional biofeedback is in any sense diminished. Rather, the rise of neurofeedback will draw deserved attention once again to the collective potential of all our self-regulation technologies.
———————
References:
Muscles Alive, Their Functions revealed by Electromyography, Fourth Edition, J.V. Basmajian, Williams and Wilkins, Baltimore).
Beyond Biofeedback, Elmer and Alyce Green, Delacorte Press/Seymour Lawrence, 1977
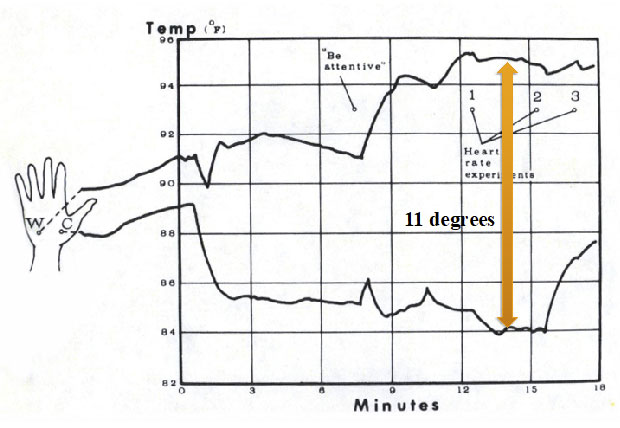
This Figure documents the achievement of differential temperature control by Swami Rama, as demonstrated to the research group at the Menninger Foundation, under Elmer and Alyce Green. Swami Rama had developed this capability without the benefit of any instrumentation, s with sole reliance on meditative techniques directed to the discernment of internal physiological states (From Beyond Biofeedback, Page 198).
———————
Siegfried wrote:
“…This distinction was brought home to me forcefully years ago when I was using temperature training to warm my cold feet.”
Like my mother, I’ve always had to wear bed socks to keep my feet warm. Swiss ophthalmologists studying the physiological markers associated with developing glaucoma bundled them up with a name. First “Vasospastic Syndrome” then variations of same and finally Flammer Syndrome.
https://en.wikipedia.org/wiki/Flammer_syndrome
Cold hands or feet, hypotension, diminished sense of thirst and increased levels of the vasoconstrictor, Endothelin-1 were some of the variables. Sure enough, my mother developed glaucoma in her old age.
Now that (like you) I’ve gotten long in the tooth, I’ve looked for ways to increase peripheral circulation and /or brain blood perfusion. Aside from certain useful supplements, I recently found the most satisfactory intervention was far-infrared emitting ceramic material. (Inserted inside fabric threads and activated by body emissions.)
After many years of trying, on July 25th a small Santa Monica, CA company that makes this stuff (there are others in Brazil and the far east using different formulations) finally received FDA approval to call it a medical device and general wellness product.
“Medical devices and wearable technology can often perform just as well as drugs, and they generally have much fewer side effects,” Dr. [Michael] Hamblin [MIT & Harvard, member of the company’s scientific advisory board] said.
“But, intuitively, by wearing something, most people do not believe it will affect their physiology. So you have to convince them.”
“It is kind of impossible to overdose on Celliant fabric, and for many other products or medicines this is not the case,” Dr. Hamblin said.
“And that’s one of the big attractions. If you wore a whole body Celliant suit 24/7 the benefits just build up.”
https://www.sporttechie.com/celliant-textile-technology-can-help-athletes-increase-blood-flow/
One of the studies (at a VA Hospital) that helped them get the FDA approval:
BMC Complement Altern Med. 2009 Apr 22;9:10.
Effect of optically modified polyethylene terephthalate fiber socks on chronic foot pain.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2680395/pdf/1472-6882-9-10.pdf
Referenced in a 2012 review of Far Infrared light radiation co-authored by Hamblin (who was a speaker at this year’s LENS Conference):
Far infrared radiation (FIR): Its biological effects and medical applications
https://pdfs.semanticscholar.org/8586/761430f1857221e8bd295a5e669713bde21f.pdf
Near and far infrared light therapy by various modalities (LED’s, lasers, heat lamps, saunas, non-thermal bioceramics) is now referred to in scientifical circles as Photobiomodulation.
At ISNR Foxwoods, I was walking around in the exhibitor’s hall with a blue long-sleeved Saucony workout shirt (woman’s small, made with around 50% Celliant material) wrapped around my head like a turban. Gary Ames asked me why I wearing it. I immediately shot back, “So I don’t have to wear a strait-jacket.”
He seemed satisfied with this reply.
Siegfried, the point of all this is to suggest that if you decide to wear socks with Celliant (AKA Holofiber) material — percentages of which, depending on the manufacturer, can vary widely — you may no longer have to use thermal biofeedback training to keep your feet warm!
Best,
Robert
Thanks, Robert. This has been very helpful.