Pain
by Siegfried Othmer | December 22nd, 2004Making a Case for the Exercise Model
We have just submitted a paper to the JNT in support of the proposition that inter-hemispheric training can remediate attentional deficits irrespective of the presenting complaints. In the back-and-forth with the editors that has by now taken some months, their frustration is apparent that we never seem to come up with the kind of data that simply nails it. If this technique is indeed as effective as we say, then why not just show some EEG data which makes this obvious. The reason we don’t show such EEG data is that we don’t wish to promote the wrong conclusion. If we showed EEG data that proved our hypotheses, then an EEG criterion or EEG litmus test would follow, which would be a mistake in our view.
Rarely do we have the chance to prove this to the world, since we don’t bother taking a lot of EEG data any more. However, when Sue and I were writing our book chapter on pain a few months ago, we were asked specifically for EEG data, so we requested of Richard Soutar to send us a case with EEG data that we could include.
He sent us a case of MS and Fibromyalgia of long standing. In line with the normal procedures at that office, a QEEG was obtained at the outset. The outstanding feature was a pronounced excess in EEG amplitude at 13 Hz. In consequence, EEG normalization training was undertaken at 13 Hz. After some five sessions, this was abandoned because no clinical response had been obtained. The EEG status at session 5 is shown in Figure 1 below. Instead up-training of the alpha band was undertaken, even though no EEG anomaly was seen in the alpha band. With each of the early sessions, the patient experienced pain relief for two days after the training. After session #12, the pain-free period extended for a whole week, and after #16, it was two weeks. After session #29, he was essentially pain-free steady-state, and by session #50 he was also off Zoloft.
The EEG after session #29 is shown in Figure 2 below. Curiously there is no change observed in the training band of 10 Hz. Yet amplitudes have significantly normalized in the 13-Hz band. This makes the case about as well as we can for the exercise model. The changes induced by the EEG training are non-local in the frequency spectrum, and no change in the training band is required as “proof” that the neurofeedback was effective.
Soutar also sent us data on coherence. The data at session #5 are shown in Figure 3, and the data at session #29 are shown in Figure 4. Curiously, the coherence anomalies are nearly all resolved with the exception of the training band itself, where coherence measures have arguably gotten worse. Hence, the neurofeedback effect is non-local in the spatial domain as well. If training had been done according to EEG criteria, the alpha training would not have been undertaken in the first place, and on the basis of the coherence data would not have been continued for very long. Yet it was apparently more effective in addressing the anomalies in the 13-Hz band than 13-Hz down-training itself.
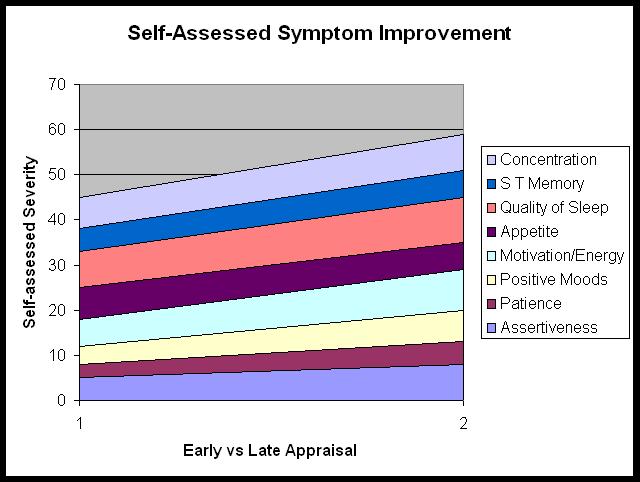
Symptom change is tracked in Figures 5, and aspects of function expected to improve with training are shown in Figure 6. It will be observed that the patient still indicates a certain level of pain at the post-assessment, although he describes himself as “pain-free.” One suspects that this has to do with the actual nonlinearity of pain perception and pain severity. Whereas a level of 9 or 10 might make one reconsider the desirability of staying alive, a level of three hardly interferes with life.
At a minimum, cases like this must give us pause with respect to the narrow claim that neurofeedback efficacy must be demonstrated by means of change induced within the training band and at the training site. At another level, it must cause us to take a larger view of what we are doing. We are training brain networks. We are appealing to specific brain mechanisms, wherever these may be accessible to us on cortex and in the frequency domain. These in turn engage with other brain mechanisms, so that the end result is improved self-regulation in some considerable generality.
Since we are not necessarily inducing readily measurable change at the training site or within the reward band, the term “exercise model” seems appropriate.
Figure 1
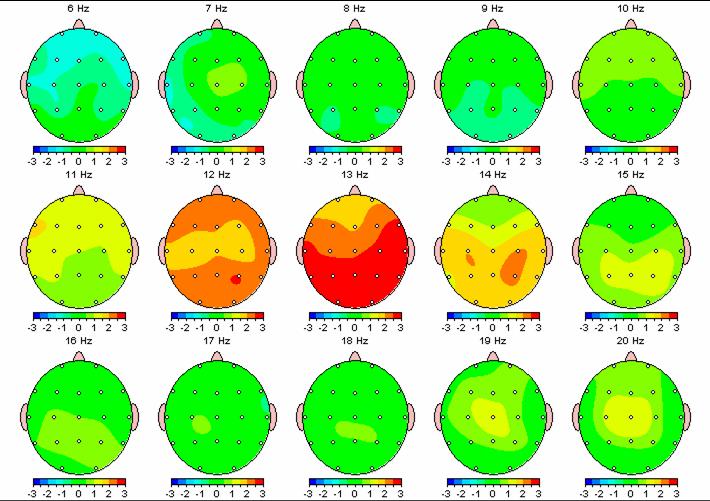
Figure 2
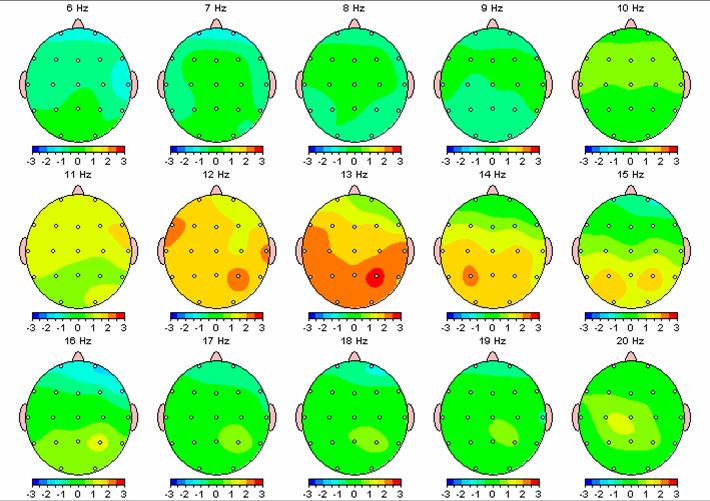
Figure 3
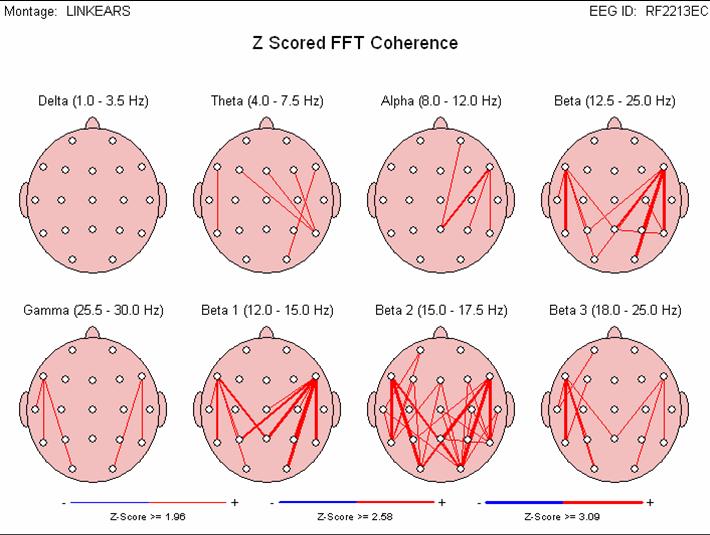
Figure 4
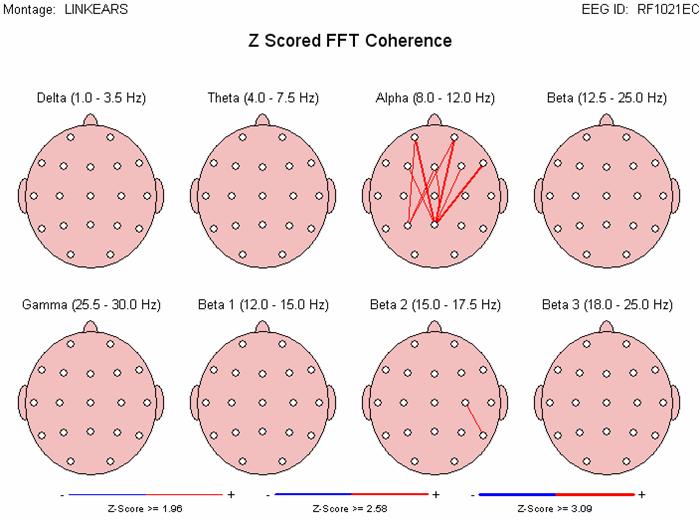
Figure 5
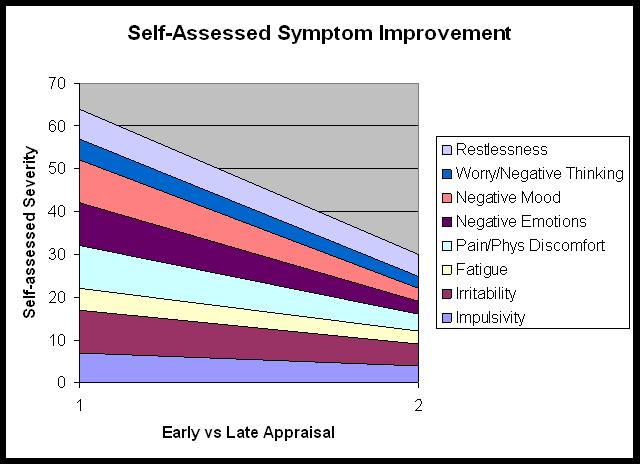
Figure 6