





A Remarkable Recovery
by Siegfried Othmer | April 28th, 2017By Siegfried Othmer, PhD
After more than thirty years in neurofeedback one is less likely to be surprised by a particular clinical outcome than in an earlier day. A few months ago Kurtis Walton sent me a set of pre-post QIKtests (CPT) that showed startling change where that had not really been expected, so that is worth a further look. The client has given her permission for us to present information on her experience with the training.
At issue here is one of those classic cases of early trauma that sets a person up for what we call the “disregulation cascade,” in which every subsequent traumatic event exacerbates the prior condition, worsens the disregulation, and sends the person ever further into dysfunction. Infra-Low Frequency Neurofeedback is the remedy of choice for this condition, but just because remediation is possible in such cases does not mean that it is straightforward. A lengthy journey is often in prospect, although one does get to see some daylight right from the beginning.
The client does not remember much from her childhood, which often signifies suppressed trauma memories. There were attachment issues and the parents divorced when she was twelve. The client had two head injuries related to domestic violence, and was now suffering from major depression, fibromyalgia, and panic attacks, among a litany of other symptoms. There are extremes of visual and auditory sensitivity.
The training was challenging in particular because the symptom presentation was so pervasive that it was difficult to chart a path forward in the usual fashion. The first task in Infra-Low Frequency (ILF) neurofeedback is to determine the Optimum Response Frequency, and that becomes a challenge when the client is really not in a position to judge one way or the other. This is not uncommonly the case with fibromyalgia and other cases of chronic pain. When pain levels are at an extreme, subtlety gets lost, and the client is unable to discern a ‘good’ place to train. The ORF was not finally established until much later in the process. That was not a barrier to progress in training, however.
The client was coming from some distance, in Alaska no less, and so training was done intensively in batches, at three sessions per day four days in a row. At session 36 the QIKtest was re-administered and a surprising degree of progress was demonstrated. At the same time, however, the client was still suffering from a raft of symptoms, which had kept expectations for the CPT results modest.
In the QIKtest we distinguish between two kinds of measures, the discrete errors (errors of omission; errors of commission; and outliers in reaction time) and the continuous variables of reaction time (RT) and of variability (the spread in RT). The first gives us a measure of accuracy; the second a measure of relative performance.
In the initial QIKtest (given in this case after the very first ILF training session), the client had scored in the first percentile range on the accuracy measure. There was no problem with errors of commission, but a high rate of omission errors and of reaction time (RT) outliers was observed. At the 36-session re-test, there were no discrete errors at all. None. The client had moved from scoring in the first percentile range to performing at the 99th percentile in accuracy. At the same time, although symptom relief was being experienced, one would not wish the client’s existing state of distress on anyone. With respect to the critical issues here, the training was nearer to the beginning than to the end of the process. With regard to progress in the performance measures, the client moved from the second percentile to the 37th, a substantial improvement under the circumstances.
Now it is not at all unusual for us to restore people who are starting out in the first percentile bin in terms of accuracy to the normal range of function or above. That’s actually what we expect to accomplish. And it is also not unusual to take people starting out in the normal range to the very high performance levels. But it is indeed unusual to find a person moving from the first percentile bin to the 99th percentile bin, particularly when in so many other respects the person remains in a state of profound disregulation. It is worth drilling down further to see just what makes this situation special.
First of all, it is not unusual for the training to take adults to the point where they make no omission errors and exhibit no outliers in reaction time. That is the expectation for normal adult function and we expect to attain that level of function fairly routinely. What keeps most adults from a perfect accuracy score are the commission errors. Life is more forgiving of errors of commission than of omission, and so in a pressured reaction time test we typically bias our performance to the point where we ‘accept’ a certain risk of a commission error in order to stay poised for a rapid response. In this instance, however, the client was not making many commission errors even at the outset. There had been only one such error in the pre-test. This already testifies to a certain level of functionality that this person was able to retain despite all of her trials and tribulations. The training then simply had to build upon that foundation.
On the other hand, such functionality was only apparent in that particular measure, not in the observed behavior in general, as captured in the test. In Figure 1, the time series of reaction times is illustrated for the high-demand segments of the test, and these results are not pretty.
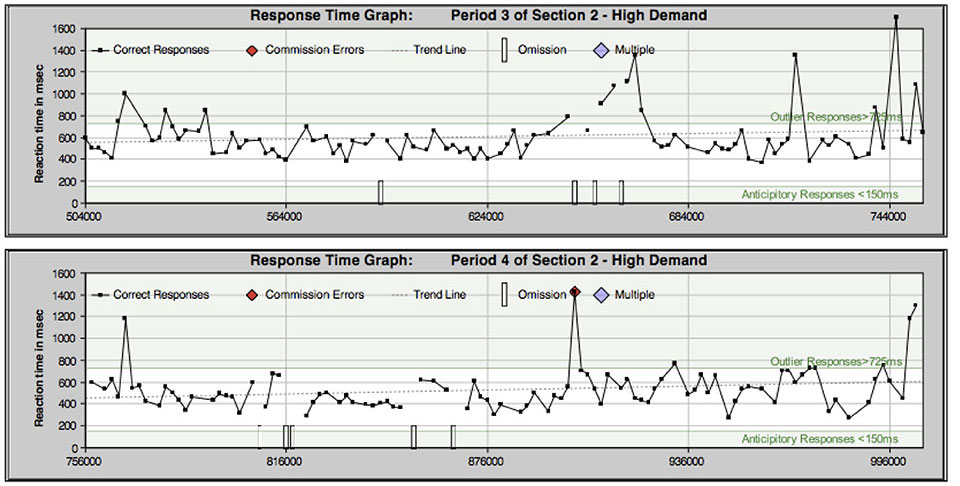
Figure 1. Time series of reaction times for the high-demand periods, pre-training.
Training proceeded fitfully as the client was able to make the trip, and then a second re-test of the QIK was performed at session 56. The accuracy score remained at the 99th percentile as before, as the client had once again scored zero discrete errors. The discrete errors are shown in the form of a stacked chart in Figure 2. (This is chart is often the most significant for the neurofeedback client.)
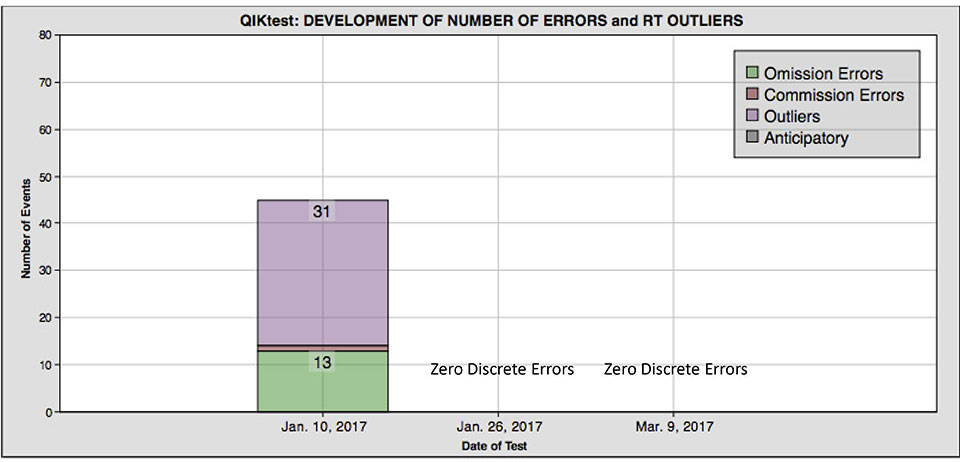
Figure 2. Stacked chart of the discrete errors for each of the three tests.
By this time, the performance score had been raised to the 82nd percentile level. The results are shown graphically in Figure 3. This degree of improvement was just remarkable, given the context. As before, the client was still suffering significant psychic and physical distress, even though progress was continuing.
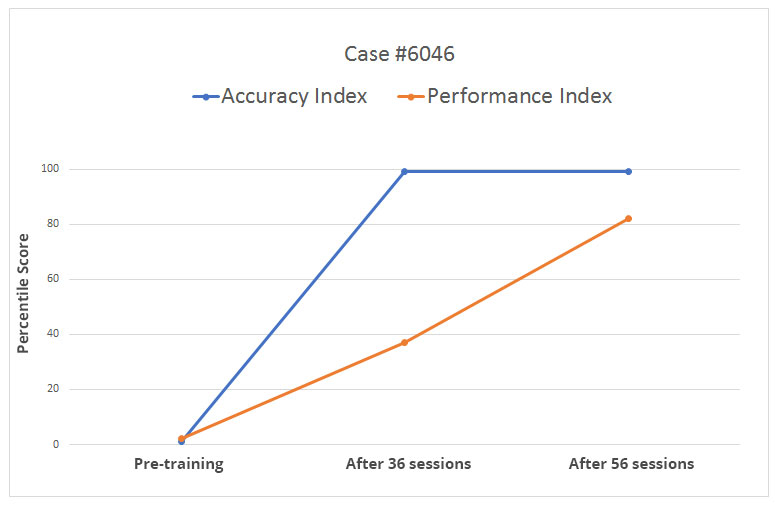
Figure 3. Percentile scores for the top-level categories of accuracy and performance for the three tests.
The equivalent chart in terms of standard scores is shown in Figure 4, along with the constituent scores for each of the top-level categories. In this compilation, the reaction time outliers and omission errors are treated as equivalent, and as such they can be combined and thus normed jointly to yield the attention index.
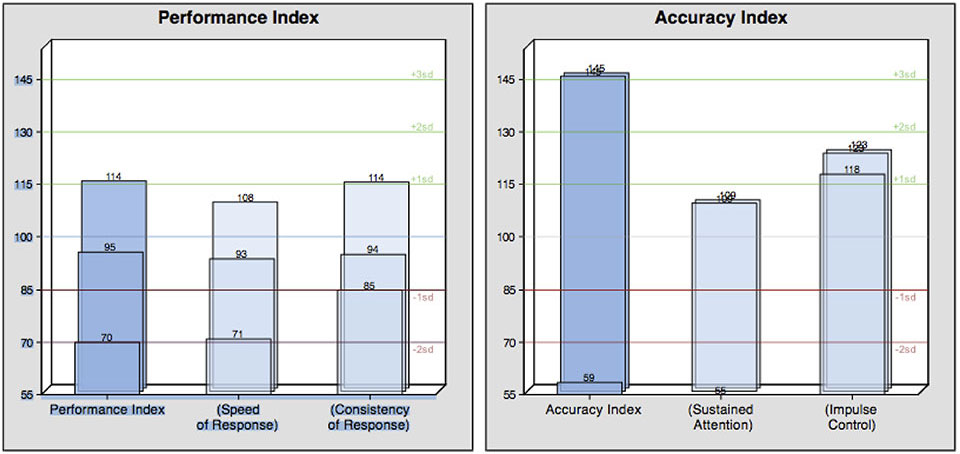
Figure 4. Chart of standard scores for the top-level categories and the subsidiary scores for the three tests. 100 is the norm; 15 is the standard deviation; and 145 is the highest permissible score allowed under the test.
It is worth noting that the excellent performance with respect to errors of commission is being retained here even as the client migrates to much better reaction time performance. This is not a surprise to us, however. We have known for many years that good performance on commissions need not be purchased at the expense of slowed reaction times. There is no necessary trade-off here. A person is in a position to choose to be more careful in the test, and thus reduce the risk of commission errors at the cost of reaction time (even though that would be in violation of the instructions for the test). But it is not necessary to give up speed for accuracy. Evidence for that proposition has been plentiful over the years.
The time series of reaction times for the high-demand periods are shown in Figure 5, and makes for a nice contrast to Figure 1. The client is now in possession of a much more functional nervous system.
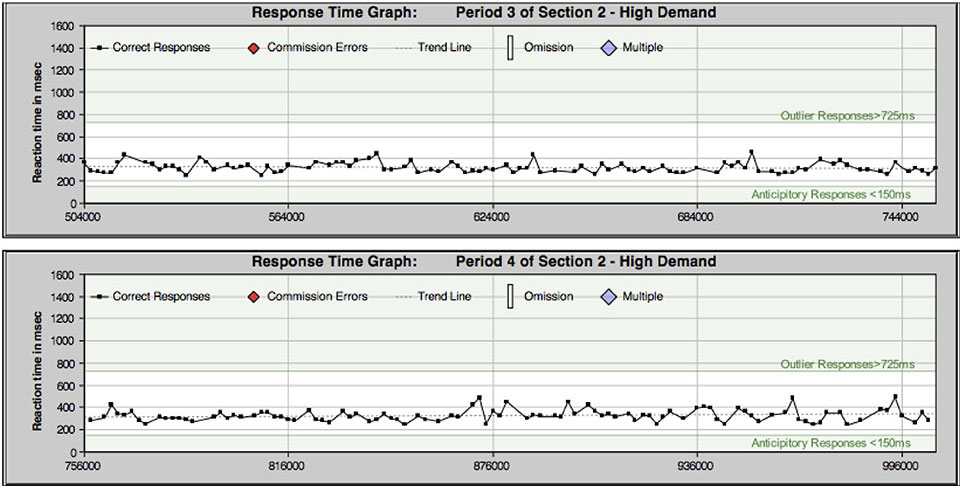
Figure 5. Time series of reaction times for the high-demand periods, for the third test, taking place after 56 sessions.
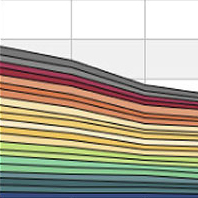
The cumulative RT distributions are shown for all three tests in Figure 6. A remarkable consistency in RT is displayed here in the third test compared to the first (and yet there is still room for further improvement).
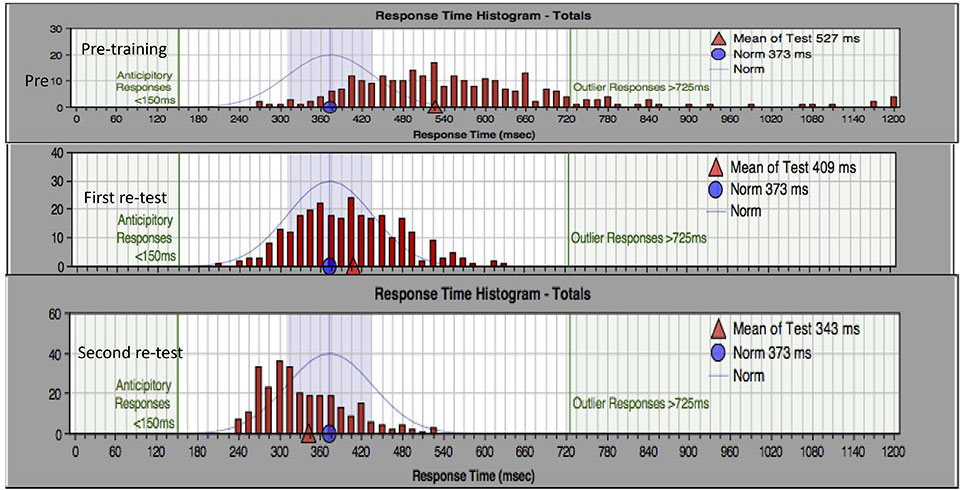
Figure 6. Pre- and post- response time histogram for the total test, including both high-demand and lowdemand segments.
It has been an implicit assumption on our part over all these years that the CPT serves as a kind of overall quality index on brain function. That is because the functionality being tested is so basic. And over the years, the proposition has been substantially supported, so we perform the test on every client capable of taking it. But one can take this argument only one way. We can say that one cannot lay claim to having good brain function unless the CPT scores are normalized, but high CPT scores are not predictive of general progress in training.
It has been a further assumption that when right-hemisphere-dominated function is compromised, then left-hemisphere-dominated function will likely be impacted as well. That was certainly the case here, but that doesn’t mean recovery takes place at comparable rates for the two kinds of functional deficit. This observation can be confirmed with Figure 7, where overall progress in symptom severity is indicated. By the time of the first QIK retest, global symptom severity had declined to 68% of the pre-training value, and by the time of the second re-test it had declined to 38%.
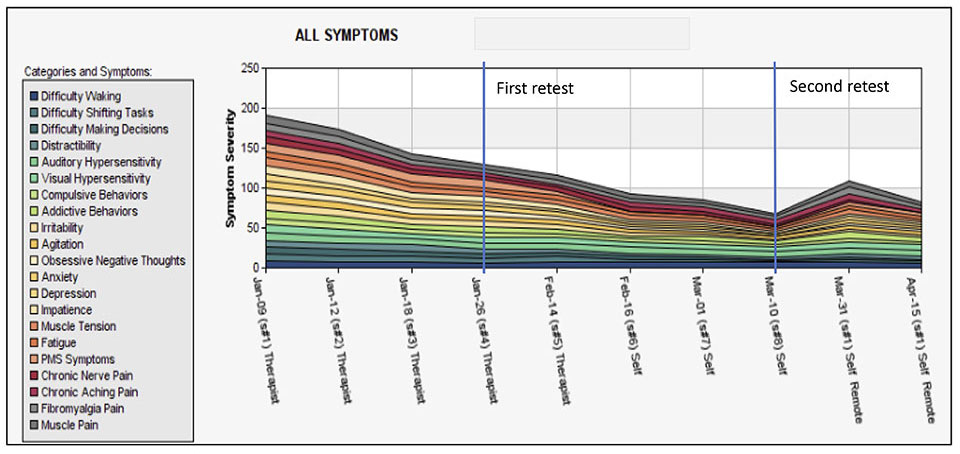
Figure 7. Symptom tracking chart, reflecting progress as assessed with a Likert scale of 0-10 for each symptom category.
It should also be noted that by the end of March, relevant medications had been discontinued. This includes Klonipin for anxiety and Gabapentin for depression and OCD.
Discussion
It is the substantial difference in rates of recovery of left- and right-hemisphere dominated function that makes this case so interesting. The differential recovery rate is even more noteworthy when it is considered that throughout the training so far the primary protocols have been targeting right-hemisphere-dominated regulatory mechanisms of core regulation. It seemed natural then to assume that improved LH function would follow in consequence of better RH function. But that’s not what happened.
It may simply be the case that there was not much of a barrier to the recovery of LH-dominated function, and so that was observed first. After all, we are accustomed to seeing differential rates of recovery for different symptom classes. LH-training seems to be a more pure case of brain-training, whereas RH-training involves the entire person much more intimately and so that becomes a much more involved task. Nevertheless, one is entitled to hope that in view of the rapid recovery of LH-dominated function there are good prospects for the recovery from the cardinal symptoms as well. We await further reports.
In reflection on these data, it is clear that in this instance having the QIKtest results available was not only inspiring to the therapist who was fully engaged with a very complicated symptom presentation, but it was also galvanizing and motivating for the client who was still mired in symptoms throughout this period of time. Even for a person not versed in technical matters, it can be reassuring to have data on functionality at hand that can lay claim to some objectivity.