





Brain Scans as Mind Readers? — Commentary on an Article in Wired Magazine by Daniel Carlat
by Siegfried Othmer | June 5th, 2008
 Neurofeedback is reaching the threshold of mainstream acceptance, so we are going through a kind of ‘darkness before dawn’ phenomenon right now where critics are at their most strident. My inclination is increasingly to ignore these criticisms and attend to the business of growing the field, but inevitably the criticisms grate, and they evoke the urge to respond.
Neurofeedback is reaching the threshold of mainstream acceptance, so we are going through a kind of ‘darkness before dawn’ phenomenon right now where critics are at their most strident. My inclination is increasingly to ignore these criticisms and attend to the business of growing the field, but inevitably the criticisms grate, and they evoke the urge to respond.
This is particularly the case when the source of the criticism comes from the most disinhibited technology enthusiasts, the producers of the magazine Wired. When a writer recently approached them about doing an article on neurofeedback, the editor asked what event or new finding would make such an article relevant at this particular moment. The fact that the magazine has never dealt with neurofeedback at all was not seen as an oversight needing correction.
With that background, one might well ask what new finding or event might have triggered them to have Daniel Carlat write an article that trashes fMRI, SPECT, and QEEG as essentially useless. “Don’t believe the hype,” says the subheading, which is strange coming from a magazine full of hype that is impossible to assess at the time of printing. The ‘hype’ in this case relates to functional imagery and its potential role in psychiatry. The article does not touch on neurofeedback.
The criticism, quite plainly, is that these new imaging tools do not seem to be the Holy Grail for resolving issues of diagnosis. But this is not a proposition with which the proponents of functional imaging necessarily disagree. Once one is confronted with the complexity of these images, the question of whether someone is or is not depressed is really no longer the pressing issue. The imagery is the point of departure for asking a lot of questions that one would not know to ask in the absence of imagery. As Daniel Amen says, “SPECT does not give you the answer; it teaches us to ask better questions.”
Has the value of this imagery for clinical decision-making been over-hyped? Surely, and we have been among the critics the whole way. But Carlat’s criticism is more thorough-going. He seems to be much more at home with the critics of these techniques who seem to be dismissing them rather wholesale. At the same time, Carlat has ignored the best evidence that can be brought to bear in their favor.
For example, Suffin and Emory have developed a program that predicts medication response on the basis of QEEG information. This program essentially bypasses the issue of diagnosis. The EEG pattern indicates what medications will help a particular brain toward more functional states. The intermediate step of diagnosis is oblique to this issue and is therefore superfluous. Now this approach can fail too. We’re in their neighborhood, and we have seen clients from their office where the technique has failed. But on balance, the technique has demonstrated predictive utility.
As another example, consider the work of Christopher deCharms on managing chronic pain with fMRI-based feedback. As a practical remedy for chronic pain, I suspect that the method will turn out to be completely impractical and unaffordable. But as a scientific step forward, the experiment was quite clean and unambiguous, and very much to be welcomed.
As for SPECT imagery as done by Daniel Amen, we have had salutary results with it for a number of purposes. On one occasion, the imagery persuaded a very skeptical father that his son was not just acting out willfully but was in fact living with serious brain-based functional anomalies. He was persuaded to allow his child to do neurofeedback / EEG biofeedback. On another occasion recently, we used SPECT imagery to document change with neurofeedback in a veteran with PTSD (see article: EEG Feedback for Post Traumatic Stress Disorder). The question of whether the imagery could distinguish between full-blown PTSD and an ordinary anxiety disorder was not on the table.
On one occasion years ago Amen got to see a young patient who was wearing Irlen lenses in order to be able to read. SPECT imagery with and without the glasses confirmed the difference, thus providing additional evidence not only for the Irlen hypothesis, but for the lenses as a categorical remedy. The only other such evidence was furnished from magnetoencephalography, another functional imagery technique. Where else would such evidence come from, one might ask. No structural deficit could ever be identified in Irlen Syndrome.
These are cases in point for the kind of clinical utility that Daniel Amen claims for his methods. Most importantly, of course, the imagery allows Amen to predict medication response in a manner similar to that of Suffin and Emory. Over time, the data are seen to fall into patterns that correlate with medication response. There is a gradual learning curve that eventually allows imagery to be classified almost at a glance by the skilled observer. Frequently the technique identifies medications that are a poor match to the condition at hand. This is not surprising. Most of the referrals to the Amen clinics are people who have not responded well to standard, formulaic treatment of presumptive diagnoses, and they are now taking the next step.
Critics belabor the point that group differences, even when these are statistically robust, don’t equate to high predictive power. This is quite true, and I have flogged this issue as well. In the clinical world, the answer lies in summoning multiple, independent lines of evidence to see if there is a correspondence. In practice, the imagery is not to be evaluated independently of what else is known about the patient. The imagery does not stand alone. This can never satisfy the skeptical scientist (Robert Rubin of UCLA in this case), but it does address the issue of low predictive power.
The final piece of evidence becomes available when the patient responds to the new regimen of meds. The medication response is then the last confirming piece of the puzzle. Each case is also yet another contribution to the collective learning curve. The clinician gathers evidence over all patients and over all time. This may disturb the hard scientist whose brain doesn’t work that way, and who feels strongly that key scientific milestones were missed along the way. That may be so, but we are beyond that point now both in functional imaging and in neurofeedback. The collective wisdom acquired from reading over 40,000 SPECTS exceeds the information value that can be derived from any formal study. The collective experience of thousands of neurofeedback clinicians by now encompasses more wisdom than is reflected in all of the formal studies.
In pursuit of the QEEG, Carlat visited both E. Roy John’s laboratory at New York University and Marc Nuwer’s office at UCLA. The main criticism was the familiar one: Run enough tests on the EEG, and some of the numbers will turn out to be statistically significant. Also, correlations with clinical disorders have not so far panned out, according to Nuwer. The best test of that hypothesis, according to him, was a “total failure.”
So does this mean the game is not worth the candle, or does it perhaps mean that the imagery indicts our prevailing concept of monolithic diagnosis. Right now much of mental health diagnosis is rather tautologous. The patient comes in feeling depressed and gets labelled with depression, or he is inattentive and gets labeled with ADD. As Amen mocks the process, if a person comes in with chest pain, we don’t give the diagnosis of chest pain. The same thing goes on in neurology. The mother of a child with CP complains that the neurologists mostly parrot back what she has just told them, only using bigger words.
The imagery data are certainly valid at some level. The questions relate to the interpretation of the data. If the data don’t match up with a rather simple-minded, tautological diagnostic edifice, does one throw out the data or perhaps take another look at the simplistic model? Since the data don’t fit the binary choices provided for in the diagnostic model, perhaps they mandate a multi-dimensional characterization that is much closer to the way complex systems actually behave.
One answer to the lack of diagnostic specificity that is already implied in Suffin and Emory’s work is that of physiological subtypes, or phenotypes. These phenotypes also exist in the ‘normal’ population, and are not simply a function of pathology. The medication response, then, may be largely a matter of the phenotype, quite independently of other issues. If this holds up, then for example one phenotype might respond much better to stimulant medication than the others, quite independently of whether the person in that cohort actually ‘has ADHD.’
 |
|
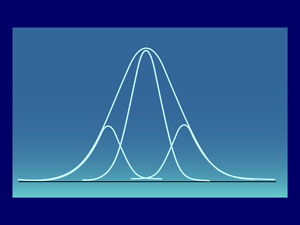
Figure 1
|
In the phenotype model, characterizing deviation from the mean now refers to the phenotype mean rather than the global mean, which changes everything in the analyses. This is illustrated in Figure 1. A person may well be more than two standard deviations removed from the global mean, but yet be within one standard deviation of the phenotype mean. This model may get us out of the bind of simple-minded diagnosis, or it might involve us in endless refinement without ever reaching closure. But in the absence of imagery, these questions could not even be entertained.
Given the dim view that Carlat takes of functional imaging, what does he recommend? He seems to have no difficulty with the standard CT scan and the standard MRI, both limited to imaging brain structure. The problem all along, of course, has been that CT scans are incapable of telling the difference between a living brain and a dead one. That hardly recommends it for telling the difference between a functional and a dysfunctional one. Yet it has been consistently relied upon to characterize traumatic brain injury over the years, with the result that the field of medicine has been in a massive state of denial with regard to head injury symptoms of which people complain consistently. If they did not show up on the CT scan, the symptoms were typically dismissed and the poor blighters were sent home. This is the main reason our society is back on its heels with regard to the huge numbers of blast injury victims coming back from Iraq. We’ve been ignoring similar problems in the civilian sector for decades.
 |
|
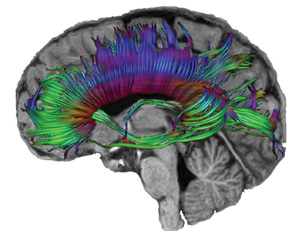
Figure 2
|
With functional imaging, these kinds of mild head injuries can be documented. Most recently, Diffusion Tensor Imaging (DTI), a refinement of fMRI, has been used to reveal functional deterioration in adolescents who are clean on CT scans, have the highest Glasgow Coma Scale rating of 15, and yet complain of post-concussion symptoms. (Wilde 2008) This kind of functional imagery is the key to progress within medicine on this condition. A representative DTI image is shown in Figure 2.
We have had comparably persuasive evidence from QEEGs for many years, of course, but Nuwer has been one of the key influences in keeping controversy boiling in that endeavor—as a paid mouthpiece for the well-funded insurance companies whose interest lies in the denial of care for victims of head injury.
We who have been working on these ‘non-existing’ symptoms with the ‘unrecognized’ technique of neurofeedback with a high degree of success over the years realize that minor traumatic brain injury represents a stealth condition of pervasive incidence within our population. Perhaps time is now finally going to be running out on this insurance company racket, a development that could only occur with the insights gained from functional imagery.
In reflecting back on this whole line of criticism, it is apparent first of all that Carlat approaches this issue in a gladiatorial frame of mind. The Wired piece reeks of partisanship. And indeed Carlat is a practicing psychiatrist, a member of the very community that is being challenged by Amen’s and John’s and deCharms’ work. Partly this is explainable as a simple human reaction by Rubin and by Nuwer to having been upstaged. And partly it is a reflection of the fact that nearly the entire field of psychiatry has been so absorbed by the pharmacological model that it doesn’t yet realize the important conversation going forward needs to be about networks and their organization in the bioelectrical domain.
The closer imagery gets to reflecting real-time information, the more apparent this becomes. And the EEG gives us the highest time resolution (along with MEG) of all the imaging techniques. The battle about the importance of the EEG is really just a continuation of the old battle about ‘the soups and the sparks.’ Because of pharmacology, the guys in the soup kitchen won the first round. The second round will take place on another playing field entirely. That playing field cannot be wished out of existence. The power of imagery will be one of our greatest assets–often going far beyond the intrinsic scientific merits! So the critics have a point, and I even share many of their concerns. But the power of imagery will just swamp the criticism, time and again. In fact, it has already done so. The world will no more slow down for Rubin and Nuwer than it did for Barkley and Ratey. They can still intimidate the mainstream of their profession, which is characteristically risk-averse; they can no longer restrain the frontier.
That frontier has not been dependent on NIH funding or even university or large-scale corporate support. Daniel Amen, as one example, bootstrapped his entire operation. He was even his own publisher at the outset. The whole field of neurofeedback came into existence through boostrapped organizations. With the movement toward functional medicine, we are entering the era of the democratization of health care–accessible, affordable, and understandable to the lay-person. And in its essence it will be oriented toward enhancing function rather than on eradicating disease. Diagnosis, which is what this entire controversy wraps around, will be largely irrelevant to this entire enterprise.
Share your thoughts in the comments section below.
Resources:
Brain Scans as Mind Readers? Don’t Believe the Hype, by Daniel Carlat, Wired Magazine, June 2008, pp. 120-128
Daniel Amen response: http://amenclinics.com/wp231/?p=47
Reference: E.A. Wilde, et al, Diffusion tensor imaging of acute mild traumatic brain injury in adolescents, Neurology, 70, p 948-955 (2008)
im not the smartest chap on the block but i have noiticed something big.
i do have a mild TBI but that doesnt mean im stupid just handicaped to a degree. i dont want to sound crazy but 80% of every media imaginable except for the net (for now) is owned and controlled. its owners dont want anything competing against there monopolies in all areas wether it be big pharma, biotech, energy, economics, banking, politics, war! all parts of the mainstream is corrupt and controlled this has been for centuries and further back even. its not just a few critics punishing promising treatments the whole system is. i know what we are fighting and so many are waking up also now thanks to the internet. im hoping some of you will bother to investigate for your selves what im talking about here.
the american government takes half the private sectors money a total of 47% there abouts. thats 50% of the countries money being controlled by beuracrats. inefficent, wasteful and corrupt government which 100 years ago only 9% was taken from the private sector. 100 yrs ago a small government with endless freedom (91%) in the private sector would have allowed things like neurofeedback race to the top of promising treatments. not anymore we have medical monopolies which squash anything competing with the mainstream. a government increasing in size and control eventually leads to communism or socialism correct? communisn take all the money out of the private sector and decide everything for the public. frredom of choice is lost but in this case we are headed for a plutocracy also with this ever increasing government. the rich are getting richer and the middle class is slowing disappearing poverty and third world is approaching in the future. how many decades away is this no one knows but its comming. could even be 100yrs but yes its approaching. throughout history governments have always oppressed there people its a cycle which repeats itself. yet we are unaware of this. we are not aware what we are heading for in this world.
our politicians are being lobbyed by massive corporations to change laws that work in there favour. these are the tools the corporations have and they “are” the mainstream remember, they are changing the country to suit them. while we the little people pass no laws we sit back and watch our right s and freedom being stripped away. you can see this in medicine our choices are norrowed to medication surgery chemo and alike.
if neurofeedback gets any reconition i believe it will be regulated and made to function at a subordinate level thanks to the influence of the pharmacuitical companies and mainstram in general.
but its not these big corporations and governments who are to blame its something even more sinister above all this. what is it that we are actually fighting?
all these great alternative treatments comming of age yet the mainstream ignores and stamps out most if not all of it. who is doing this what are we really fighting does anyone even know? bacause it ant just big drug companies. all of the mainstream in every area of life is just as corrupt and dangerous as it is in medicine. its a giant misinforming machine so dam corrupt the whole system is hijacked. madness you say this man has bi-polar and is in a manic phase. but i ant im just a little foggy minded oh do i hate this foggy head, you dr’s have your heads down busy on your work you dont have the time to investigate the root cause of the problem. want to know who we are really fighting? watch this short 47 minute documentry and this is only a “intro” to the problem i repeat “INTRO”. we are facing a huge problem so so huge. i ant mad this really is based on facts not some crazy conspiracy.
http://video.google.com/videoplay?docid=-7065177340464808778&sourceid=docidfeed&hl=en
a documentary called “monopoly men”. its based on facts not fiction and the intelligent dr would see right through this if its fake you will know it would you not . its not fiction i hope some of you listen.
those who control and print the currency of a nation control the nation, control the corportaions, control the media, control everything the government also is only a puppet. unlimited money wealth beyond your comprehension will buy you the world itself. who controls a nations money supply? this is very sad situation for us all but finally the truth is making its way thanks to the internet. remember i said this is only a intro google vidoe has tonnes of documentries on this subject so does youtube. much brilliant researches have studied it tonnes of literiture out there. research futher if you have the time. at least you americans have a Ron Paul presidential candidate trying to shrink the size of government and abolish the federal reserve return control back to the private sector. return gold and silver as legal tender. but the mainstream even squashed him and made him appear idiodic yet he is quite brilliant. your only hope i think. hopefully enough of us wake up and educate each other.
yours truely Mr TBI.