
The utility of EEG feedback or Neurofeedback in the resolution of Post-Traumatic Stress Disorder has already been established in research going back more than a decade. We now use it routinely with veterans in connection with our volunteer services (through Homecoming4veterans.org ). The world at large, however, remains to be convinced of the superiority of EEG feedback in the resolution of PTSD.
Establishing EEG feedback more generally as the treatment of choice for PTSD and other mental health issues is now an urgency, given the recent estimate by the Rand Corporation that some twenty percent of Iraq and Afghanistan veterans are coming home with major mental health concerns and/or traumatic brain injury.
To that end, we recently had one of our veterans undergo SPECT scans before and after EEG feedback training to document the resolution of the condition. SPECT is one of the standard functional imaging tools that are now available to characterize brain function and to do so relatively non-invasively. A small amount of radioactive material is injected into the blood stream, and where that activity is picked up in the brain shows the regions that are most strongly activated. PTSD characteristically shows a kind of diamond pattern formed by elevated activity frontally at the anterior cingulate gyrus, laterally at the basal ganglia, and centrally at the thalamus.
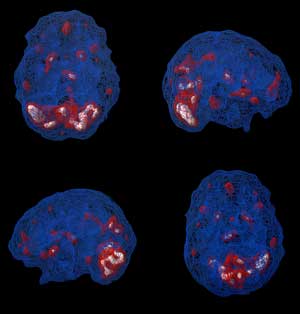

This pattern is indeed seen in our veteran, as shown in the attached Figure. After the EEG feedback training, the activity levels are much diminished, as seen in the second of the two Figures. It was already obvious from the verbal reports that matters were much improved, but it is nice to have the confirmation from the SPECT scan. The imagery also shows excess activation at the cerebellum before training, and much reduced activation afterwards. We may not know the specific functional implications of this cerebellar over-activation, but the downward trend is welcome in any event.
After sixty sessions of 30 minutes each, there were no more nightmares (or more correctly, nocturnal flashbacks); there was reduced anxiety, depression, and irritability. Sleep was improved; he was more comfortable socially, and he was drinking less. He felt more optimistic; was making plans for the future; and he was returning to school. He said that he was feeling more confident, and was happier. It is difficult for words to describe the magnitude of the change. At the time he came for training, he appeared to have very little care even about whether he lived or died. His life was not going anywhere. With respect to that benchmark, he was in a very different place after the sixty sessions of training. Moreover, he recently returned for additional sessions.

Neurofeedback & PTSD – Watch Video
Therepeutic Applications of Neurofeedback:
Post Traumatic Stress Disorder (PTSD)
—-
Siegfried Othmer
Ph.D., B.C.I.A.C.
Truly amazing side by side results.
Greetings..
I’m very pleased to see that neuro is being successfully used in treating war vets.
However, my concern is with developmental trauma for which I see precious little mention of in neuro circles.
How does one with complex trauma (developmental origin) even shop for a practitioner?
If I understand the terminology well – which I’m sure I don’t (being an educated layman) – complex trauma of a developmental origin (whether single issue or relational) presents both a stability and a regulation issue for the practitioner.
How is this best handled?
Another problem I have is that most professionals – even within the field of traumatology – seem to assume that PTSD presents only as an overaroused condition, with an over activated sympathetic NS and rapid cycling between emotions.
But PTSD can also present as underaroused with parasympathetic activation and increasing amounts of fatigue, torpor and fogginess at all levels of functioning. Sympathetic activation exists but is blanketed and numbed out of awareness.
As a veteran of trauma therapy, I found that the weak link was an effective treatment for trauma on trauma’s terms, i.e., a treatment along some kind of physical line, somatic, visceral or cortical.
I’m convinced that neuro is the best kind of treatment along those lines but as a consumer I’m very frustrated by an inability to gather enough information in order to make a good informed decision as to what kind of modality I should choose.
I’m still in the initial stages of exploring neuro (I’ve tried some coherence training but to little good effect).
I will continue to shop around for other modalities within neuro and am quite optimistic.
I also have had an amazingly good result with HeartMath’s emWave heart rate variability biofeedback device. It’s way more than a relaxation device; its more about coherence. Coherence between sympathetic and parasympathetic and between heart and brain. The heart connects directly to the medulla, thalamus, amygdala and the lower portion of the frontal cortex.
An amazingly potent little machine. (One can also get it in a PC version).
Thank you for your nice post.
Neurofeedback works just as effectively with developmental trauma. One impediment is that developmental trauma is often not identified and treated as such. It ends up masquerading under other labels. But neurofeedback is clearly effective here—which is to say, the brain is quite capable of resolving trauma under the appropriate reinforcement in both children and adults. Another point is that those who suffer most from adult trauma may very well have been “set up” or “primed” by early childhood trauma experiences. In solving one problem we are resolving the other because the mechanisms are common to both.
One advantage in neurofeedback is that the technique is non-verbal, so no one needs to be able to either articulate the problem or even label it properly. We just have to get the “system” working again as it should. Your favorable emWave experience actually illustrates the point. It has nothing directly to do with trauma. It does help to re-regulate the system. So the best of neurofeedback does the same, even when the clinician may not be specifically an expert in trauma therapy or even specifically targeting the trauma response.
The guidance I can give you as a consumer of neurofeedback is the following: You should be aware of the effects of the training essentially throughout the process—right from the beginning—and the effects should feel good to you in a variety of ways. Any ambiguity about whether this is the right thing to do should fall away quickly–or it is not the right thing to do! Also, you should be able to have an easy-going, frank and open relationship with the clinician. The path toward improved self-regulation should “feel right” to you every step of the way. You should not have to rely on the clinician’s judgment that “you are getting better.”
As for over-arousal as a descriptor for PTSD, we would say that holds even for the person who is withdrawn, disengaged, and foggy. It’s a trait-state issue. The perpetual status of the NS is that of over-arousal, but the person may well present as under-aroused. It is the EEG feedback itself that resolves the ambiguity for us. How does the person train? Universally, the traumatized person trains like an over-aroused person. There have been no exceptions.
But even if there were exceptions, it does not matter. It is not our description or understanding of the person that governs what happens. It is the training itself that defines the path forward. The person must feel good with the training, or it is not the right thing to do. And conversely, if the person does feel good with the training, it is the right thing to do, quite irrespective of the picture we may have in our heads of what ought to happen. In practice, we “migrate” the reinforcement parameters until we get to the point where the person feels most positive with the training (alert, attentive, yet calm and emotionally on an even keel).
If you are responding well to the emWave, then you should certainly do well with EEG feedback also. As you realize, the key to the trauma response lies in our whole body-mind, and cannot be resolved through our conscious minds alone. EEG feedback is our most revealing “window” into the whole web of regulation.
I recommend to you my longer piece on NF for PTSD at the website http://www.homecoming4veterans.org
Thanks for writing.
Siegfried Othmer, Ph.D.
Chief Scientist
thank you very much for your very detailed response to the letter addressing PTSD with trauma occurring at early age. Also for addressing consumer issues. I am potentially about to spend $2500 on this in the research I have seen is from a third-party but it was contracted by a vendor of software. This is extremely helpful. I will now check out your website. Sincerely, Mark