by Siegfried Othmer, PhD
.jpg)
The Historical Background
M any in the field are still relying on the traditional SMR/beta protocols that were our mainstay in the nineties. Of course, what was valid before remains valid, so the protocols are clearly useful for many applications. Indeed, the field experienced its “Cambrian explosion” of broad applicability to mental health in the early nineties, and all those forays into new clinical terrain were made with the traditional protocols.
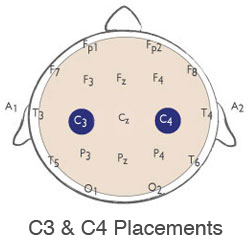
But even by the early nineties a pattern of use had emerged within the field in which hemispheric differences in response to neurofeedback were recognized. The protocol set we taught for many years came to be called “C3beta/C4SMR,” a combination that was titrated as appropriate for each individual. C3beta referred to reinforcement at 15-18 Hz at either C3-A1 or C3-T3, and C4SMR referred to 12-15 Hz reinforcement at either C4-A2 or C4-T4. The right hemisphere training was intended to be calming, and the left hemisphere training was intended to be focusing, alerting and more activating.
 When a bipolar client became manic within the session with SMR training, Sue Othmer realized that the frequency needed to be adjustable. And that led to the broad adoption of frequency optimization for work with unstable brains. These brains, in which sudden and pronounced shifts into disregulation could be observed, were our guides into the unknown terrain of frequency optimization. That was because they tended to respond in noticeable ways to even small adjustments in reward frequency within the session. Clients with Bipolar Disorder also responded exquisitely within the session, and thus the category of brain instabilities includes Bipolar Disorder as well, even though the timescale of the descent into disregulation might be large in that case. The knowledge that an optimum target frequency existed for all individuals somewhere within the EEG spectrum gave us the necessary confidence to proceed with the optimization procedure, and thus with the exploration of the entire spectrum.
When a bipolar client became manic within the session with SMR training, Sue Othmer realized that the frequency needed to be adjustable. And that led to the broad adoption of frequency optimization for work with unstable brains. These brains, in which sudden and pronounced shifts into disregulation could be observed, were our guides into the unknown terrain of frequency optimization. That was because they tended to respond in noticeable ways to even small adjustments in reward frequency within the session. Clients with Bipolar Disorder also responded exquisitely within the session, and thus the category of brain instabilities includes Bipolar Disorder as well, even though the timescale of the descent into disregulation might be large in that case. The knowledge that an optimum target frequency existed for all individuals somewhere within the EEG spectrum gave us the necessary confidence to proceed with the optimization procedure, and thus with the exploration of the entire spectrum.
It wasn’t long before the optimum reward frequency became advisable for every client, even if we had to work from session to session in order to localize it. Further work with brain instabilities led us to combine left and right hemisphere training in bipolar montage, and that has made all the difference for those applications. For years this had not made sense to us because we knew that the two hemispheres needed to be treated differentially. Of course the two hemispheres also have to communicate with each other at given frequencies, and one ought to be able to train that mechanism as well. The optimization procedure was the key to figuring this out, and it turned out that inter-hemispheric training optimized at the same frequency as the right hemisphere in each individual. One could even say that so far as the interaction between the two hemispheres is concerned, the right hemisphere plays the controlling role in matters of state regulation.
Commonalities of this Approach to Functional Enhancement
The optimization procedure led to the discovery that each individual has various optimal response frequencies throughout the EEG spectrum. Whatever the starting frequency was, there appeared to be an optimum nearby for most people. For a few people, one had to range far afield, as far as 40 Hz, to find an optimum, but this was the rare exception. The adoption of the optimization strategy led to a broad exploration of frequency space, if one surveys our clinical experience collectively. Certain patterns could be discerned. The right hemisphere remained the target of choice for calming, and the left hemisphere for activation and improved focus.
When all the data were looked at collectively, they revealed that the left and right hemispheres always differed by two Hz. This held true independently of placement within each hemisphere, and over the entire conventional frequency range. The old combination of C3beta/C4SMR differed by 3 Hz, but that was a legacy protocol that was established well before frequency specificity had been recognized. Once the rule was discovered originally, it was used clinically in a predictive fashion. When training was first moved from the right hemisphere to the left in a particular case, the new target frequency would be predicted, and the prediction then verified.
The consistency and universality of the 2-Hz difference was a remarkable finding. There is still no obvious explanation in neurophysiology for this difference. But even without the benefit of an explanation, the findings are too consistent and too universal to ignore, and so they serve to validate our claims. Consider what has to be true in order for the above finding to have been made: SMR/beta neurofeedback has been validated as a strategy for altering physiological state; the optimization procedure itself has been validated (meaning that training-induced state change is sufficient to allow the optimization strategy to be implemented systematically and reproducibly in practice). And finally, the hemispheric differential response has been validated. This represents a testable proposition that is the linchpin of our clinical approach.
We also now know that training can be fruitfully done at any frequency in the EEG spectrum. The brain is responsive to information about any EEG frequency in the classic spectral range. Hence SMR/beta training loses its special place. That is not a reason to give up on it, but good practice would suggest that at a minimum an optimization procedure be adopted with the standard protocols as a starting point. That is the strategy we followed for some years in the late nineties. It is advisable for anyone who is still relying on the standard protocols.
One additional commonality was exposed with our optimization strategy that ranged over the entire EEG spectrum: The same placements were used throughout with good effect. Now, it is not possible to claim that these placements have been optimized, since that would require yet another vast set of comparative data. But it is possible to observe that results are consistent across the entire frequency spectrum. And it can also be fairly claimed that with the few principal protocols that have emerged out of the many that were tried, rather complete coverage of the clinical terrain has been achieved. This means that one can confidently rely on the standard protocol set in any frequency range at which one chooses to operate.
Implications of Infra-Low Frequency Training for the Traditional Protocols
So where does this take us? First, let it be said that in our experience there is nothing to compare with infra-low frequency training in terms of its effectiveness, rapidity of response, and power in the hands of the clinician, within a framework of clinical decision-making that by now has been well explored. The clinical reach is quite clearly broader than what we had with the earlier methods. We are effective with much more challenging clients than before, and we are effecting change more quickly and comprehensively. But we are also aware that this method places great demands on the instrumentation, the signal processing, and the skill, knowledge base, and clinical experience of the therapist. This is very demanding work. Therapists entering this field likely have no prior experience with a technique this powerful. Many neurofeedback clinicians have apparently heard this message and have decided that this bracing frontier is not for them. They are content to work with previously established protocols. Yet others are using ILF training for all the above reasons, but have not given up on the older, higher-frequency training for specific purposes.
So what is our message to all these people about how to proceed? The basic message is straight-forward: The optimization procedure applies across the board, and the standard protocol set, as well as the protocol hierarchy, applies across the board. All of the specifics are covered in the latest Protocol Guide, by Sue Othmer (EEG Info, 2013). Not covered there presently are the frequency rules that prevail for the conventional EEG spectrum. Clinicians who venture into this higher frequency region for the first time need to be mindful that the frequency rules differ from those that prevail in the infra-low frequency region that is covered in the Guide. Across the entire range, the left hemisphere training optimizes at 2Hz higher than the right. These rules are valid down to 2Hz on the right side (hence 4Hz on the left). Below that, the familiar harmonic relationship applies, with the left hemisphere optimizing at twice the right-hemisphere optimum. The two criteria correspond at 2Hz on the right side. That is to say, 2×2 = 2+2= 4. These relationships are illustrated in Figure 1.
.jpg)
The vast majority of inter-hemispheric training, at least at the outset, will be done on the central strip (T3 – T4). For this placement, the optimum training frequency matches that of the right hemisphere. If inter-hemispheric placements are used off the central strip, then going forward on the head requires using frequencies 2 Hz lower, whereas moving back on the head means using frequencies 4 Hz lower. If one gets to frequencies so low that these formulas can’t apply any more, then instead of moving down by 4 Hz one divides by 4. Similarly for the 2 Hz case.
Some practitioners who use ILF training also invoke the higher frequency training under certain circumstances. Many of them spent years with the older methods, and these have continued to play a role in their practice. Most typically the issue being addressed is the ADHD child who may respond well to the ILF training in terms of emotional regulation, vigilance, impulsivity, and hyperactivity, etc., but who now lacks what the parents once knew as his ‘spark.’ We are now persuaded that this can also be addressed with left-hemisphere training in the ILF region, but someone versed in the old SMR-beta training may at this point draw on the older approach. As both approaches have proven effective, there is no harm in using the older, but still valid, SMR-beta protocol. Particularly if the ground has been prepared, so to speak, with the infra-low frequency training, it can be easily established whether the higher frequency training is also helpful.
Continuous Feedback at High and Low Frequencies
In the infra-low frequency region, we have to rely on waveform-following for the feedback because the frequencies are so low that one could not work on the basis of an amplitude measure. But what about at higher frequencies, where traditional operant conditioning methods are applicable? It turns out that we have historically relied on waveform-following here also, only in this case it is the amplitude envelope of the EEG rhythm that is being tracked. We have emphasized this kind of continuous feedback on spectral amplitudes in each of the systems that we have designed [NeuroCybernetics (1987), EEGer (2001), and Cygnet (2007)].
It is the waveform-following aspect that makes it possible for the brain to distinguish the different EEG frequencies so readily, and thus to make the optimization procedure possible (hence advisable, and even obligatory). It is undoubtedly this feature that allowed Sue Othmer to discover the frequency-specificity originally, even in the higher-frequency region where it was not so obvious. The process is illustrated in Figure 2, where a filtered waveform is displayed for three adjacent frequencies. Even though it is difficult to see the difference between them, the brain experiences them differently. The waveform used in feedback is shown in green for one of the signals. The difference between the waveform is somewhat more apparent in a spectral analysis, as shown in Figure 3.
.jpg)
.jpg)
The ability of the brain to discern the subtleties in the signal is illustrated nicely by a development a few years ago of the method called “Beta Reset.” This technique was developed by Jaclyn Ginsburne and Jana Harr. The strategy is to increment the target frequency in the SMR/beta band upward by a small amount every 90 seconds. Reportedly, this has the effect, among other things, of stirring up traumatic material that is then brought up for engagement by the psychotherapist. The strategy bears some similarities in that regard to EMDR (Eye Movement Desensitization and Reprocessing). The method also stimulates re-regulation in neurodegenerative conditions.
We assume that what happens here is that every 90 seconds the brain has to adjust to a new set of circumstances. The episodic interruption of its state has system-wide impacts that can stir up traumatic material (if it is available to be stirred), or just challenges the brain to re-organize. What interests us in this process at the moment is the proof it provides that the brain can apparently distinguish the amplitude waveform between two adjacent frequencies reliably within 90 seconds. The brain can tell almost immediately that the imagery on the screen no longer reflects what it did a moment ago. If this were not the case, then the Beta Reset method would never have been discovered.
We may conclude, then, that it is waveform-following that has carried the burden of our training all along. By the same token, it is the continuous feedback that is largely responsible for keeping the brain engaged with the process. Of course the discrete rewards—beeps, in our case—do matter. We know that because “beeps-only” training, with no visual input at all, works also. And we know that the inhibits contribute measurably to our success as well, because these can also be used successfully in stand-alone fashion. The brain makes use of all the information that we give it. But if the quality of our training hinges on the optimization procedure, as it clearly does, then that takes us back to waveform-following as the critical element.
Success in applying our infra-low frequency training strategy at higher frequencies is therefore contingent on a feedback representation of the dynamics in the training band, not just of the threshold crossings. Cygnet offers this capability quite well. As a matter of fact, that is what it was designed for from the outset, a carryover from our earlier designs.
Developing a Strategic Framework for High and Low Frequency Training
The discussion thus far has been at the level of tactics. It is left to imbed this combination within an overall strategic framework. Unfortunately, no comprehensive strategic vision exists at this point, or it would have been mentioned earlier in this piece rather than being brought up at the end. What we have are a set of commonalities that speak to an overall unitary quality of our regulatory regime. These commonalities were exposed in a migration to lower frequencies that by now has covered five orders of magnitude, and the clinical methods have increased in their efficacy with every further descent in frequency.
It is therefore tempting to conclude that the infra-low frequency training is targeting the foundations of our regulatory hierarchy, one that is reflected in the EEG spectrum. But even though the infra-low frequency training is comprehensive in its effects, it is not exhaustive. Higher-frequency training interacts with a more complex set of dynamics, and thus can get different things done. With the increasing specificity that comes with higher-frequency training, however, the options in terms of clinical strategies proliferate. That is what we are presently seeing within the field: It is populated by a variety of ways to organize the clinical agenda.
The commonalities that have been laid bare with our systematic migration to low frequencies could form the modest beginning of a new schema for clinical decision-making, one that rests on what has been accomplished in the ILF region. By assumption, everything carries over to the higher frequencies, both in terms of placements, the rationales for targeting, and the sequencing of clinical objectives. Whatever is found to be useful at higher frequencies in a particular case can then be a point of departure for further refinements, or additional initiatives, if necessary.
What might be considered the “common core” of the approach is first of all a reliance on bipolar montage to draw the brain’s attention to relationships between sites rather than to activity at a given site. Secondly, it is the emphasis on continuous rather than discrete feedback, in order to allow the brain to track the signal and take command of the process, as opposed to being ordered about by means of discrete rewards. And thirdly, it is the adoption of an optimization procedure based on the response to the training.
The implications of the commonality we have observed is first of all that SMR/beta training has lost the special place it had laid claim to by virtue of history and sheer familiarity. Instead, a very special place is now claimed for the deep infra-low frequency region. This is surely because the ILF training takes us to the foundations of our regulatory hierarchy, and back to the early stages of our developmental trajectory. Hence the guiding principles for moving back into the higher-frequency domain are the same: attention to the regulatory hierarchy and to the sequencing of developmental stages. This suggests a scaffolding approach, one in which we progressively move toward the higher frequencies in the spectrum, and toward greater specificity in targeting.
Summary and Conclusion
The developmental path that has taken us deep into the infra-low frequency region was based almost entirely on what we had learned in doing SMR/beta training. Looking back on that development, the commonalities that have been consistently observed throughout can serve as organizing principles for a comprehensive clinical strategy. We can return now to the higher-frequency region after having accomplished what we can with the infra-low frequency training, and thus laid the foundation for restored self-regulation. The basis may have been laid for more effective higher-frequency training. We also arrive there with a much better perspective in which to appraise progress and make decisions about how to move forward. We shall have come full circle.
“We shall not cease from exploration, and the end of our exploring will be to arrive where we started and know the place for the first time.”
– T.S. Eliot
Links
Sue Othmer’s Protocol Guide
Development of the Othmer Method (6 part Video)
Find a Neurofeedback Provider Near You
Professional Education
Online Education