Why sham feedback fails as a placebo
by David A Kaiser, MFA, PhD
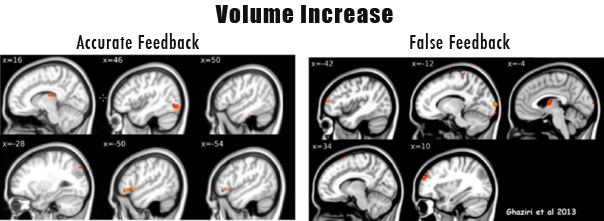
.jpg) In a recent study, truthful feedback is compared with false feedback using MRI and DTI analysis (Ghaziri et al., 2013). After 40 sessions of EEG training, both forms of feedback were found to increase gray matter volume in the brain, but veridical feedback produces twice as much new gray matter for select brain areas. Accurate feedback also increases white matter volume, strengthening connections between brain areas, while false feedback revealed no impact on connections in this study.
In a recent study, truthful feedback is compared with false feedback using MRI and DTI analysis (Ghaziri et al., 2013). After 40 sessions of EEG training, both forms of feedback were found to increase gray matter volume in the brain, but veridical feedback produces twice as much new gray matter for select brain areas. Accurate feedback also increases white matter volume, strengthening connections between brain areas, while false feedback revealed no impact on connections in this study.
Gray matter consists primarily of neurons, glia, and capillaries. It is grayish-brown in color under normal light because neurons and glia allow the color of capillaries (blood) to show through. Perhaps for that reason, it is now represented as gray in MRI imaging. White matter consists of myelinated and unmyelinated axonal pathways: wherever there are sufficient myelin-insulated axons, the area appears white, as the color of capillaries does not bleed through. The more white matter a brain possesses, the faster and more plentiful its connections, a key factor in establishing our intellectual repertoire. Myelination not only allows faster connections but briefer refractory intervals (i.e., the ability to fire again after shorter rest period), by as much as a factor of 34 (Felts et al., 1997). Irrespective of accuracy, both forms of feedback produce two or three times more gray matter volume in the untrained hemisphere (left hemisphere in this study). However, veridical feedback produces twice as much volume increase in the left hemisphere as in the right hemisphere, and false feedback produces more than three times greater increase in the left hemisphere than in the right. When truthful feedback is provided, right hemisphere volume increases 2.7 times more than in the case of false feedback.
In Ghaziri et al. (2013), 24 students at the University of Montreal underwent EEG training. Half of them received veridical feedback and half of them received false or sham feedback. (A control group for passage of time was also included.) Each group consisted of 9 females and 3 males, mean age of 22. EEG training consisted of rewarding low-beta frequencies (12-15 Hz) over the right-sided central executive network, with feedback provided using animation and songs. Placement sites (F4, P4) are above cortical connections responsible for conscious evaluation of social information, among other functions. The Central Executive Network (CEN), also called fronto-parietal network, mediates between internal and external attention, between the Dorsal Attention and the Default Mode networks (Dang et al., 2012). Given that dopamine modulates attention by coupling the CEN with our Default Mode Network as it decouples with the Dorsal Attention Network (Elsinga et al., 2006), further studies may elucidate dopaminergic changes due to neurofeedback protocols using positron emission topography (PET) (Dang et al., 2012). Training other neurofeedback frequencies such as infra-low frequency (<1 milliHz) and alpha and theta bands (8-12 Hz, 4-8 Hz) may modulate dopamine as well or other neurotransmitter systems such as serotonin and GABA.
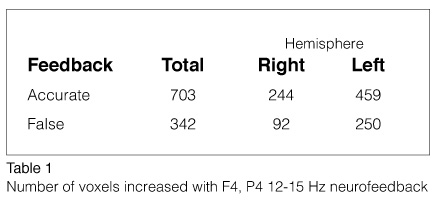
With veridical feedback, the largest increase in brain volume is reported in Brodmann Area (BA) 47L, a brain area in the left orbitofrontal cortex associated with social norms of behavior and self-generated rhythms, a critical area for speech (see Table 1). The second largest change is in BA 21/22L, where we process words and concepts and consolidate those recently encountered, among other capacities.
Reduced volume of the left medial temporal area is associated with first-episode schizophrenia (Kasai et al., 2003; Sun et al., 2009), which suggests that veridical feedback may exercise select conceptual and verbal skills, protecting us from idiopathic and psychotic ideation. Other brain areas that increase with accurate feedback are the right temporoparietal area (BA 18, 19, 37), involved in episodic and unique recognition of visual information including faces, and the right thalamus, among other areas with smaller changes.
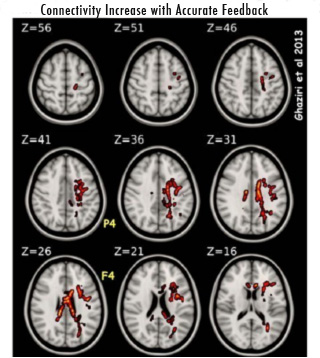
False feedback increases volume in the left primary visual cortex, where early visual categorization is performed, and the right medial prefrontal cortex, which serves intentionality and self-reflection, including identifying conflict between intention and sensory information. The increase of volume in these areas makes sense as the experimenters misrepresented the accuracy of the information for this group, and the brain was left to contend with the ambiguity of deception even while the conscious mind remained committed to the formal objective, unaware of the ongoing conflict (Deppe et al., 2005; Fink et al., 1999; Gallagher et al., 2002). Finally, right-sided CEN training increases seven axonal groups, four in the left hemisphere and three in the right. Connectivity changes are primarily intralimbic and corticolimbic. Purely neocortical connections are limited to visuo-attentive processing and motor integration of the left hemisphere. Taken together, these findings demonstrate why sham training (false feedback) is a poor “placebo” control, as false information is not inert but rather is able to set up a brain challenge that can alter brain structure, and therefore function, significantly within the time scale involved in typical neurofeedback training.
References
Dang LC, O’Neil JP, & Jagust WJ (2012). Dopamine supports coupling of attention-related networks. Journal of Neuroscience, 32, 9582-7.
Deppe M, Schwindt W, Kugel H, Plassmann H, Kenning P (2005). Nonlinear responses within the medial prefrontal cortex reveal when specific implicit information influences economic decision making. Journal of Neuroimaging, 15, 171-82.
Elsinga PH, Hatano K, & Ishiwata K (2006). PET tracers for imaging of the dopaminergic system. Current Medicinal Chemistry, 13, 2139-53.
Felts PA, Baker TA, & Smith KJ (1997). Conduction in segmentally demyelinated mammalian central axons. Journal of Neuroscience, 17, 7267—7277.
Fink GR, Marshall JC, Halligan PW, Frith CD, Driver J, Frackowiak RS, Dolan RJ (1999). The neural consequences of conflict between intention and the senses. Brain, 122, 497-512.
Gallagher HL, Jack AI, Roepstorff A, Frith CD (2002). Imaging the intentional stance in a competitive game. Neuroimage, 16, 814-21.
Ghaziri J, Tucholka A, Larue V, Blanchette-Sylvestre M, Reyburn G, Gilbert G, Lévesque J, & Beauregard M (2013). Neurofeedback training induces changes in white and gray matter. Clinical EEG and Neuroscience, 44, 265-72.
http://tallahasseeneurobalancecenter.com/Portals/0/BrainGrowthNFB.pdf
Kasai K, Shenton ME, Salisbury DF, Hirayasu Y, Onitsuka T, Spencer MH, Yurgelun-Todd DA, Kikinis R, Jolesz FA, & McCarley RW (2003). Progressive decrease of left Heschl gyrus and planum temporale gray matter volume in first-episode schizophrenia: a longitudinal magnetic resonance imaging study. Archives of General Psychiatry, 60, 766-777.
Sun J, Maller JJ, Guo L, Fitzgerald PB (2009). Superior temporal gyrus volume change in schizophrenia: a review on region of interest volumetric studies. Brain Research Reviews, 61, 14-32.
Vuust P, Wallentin M, Mouridsen K, Ostergaard L, Roepstorff A (2011). Tapping polyrhythms in music activates language areas. Neurosci Letters, 494, 211-6.
Vuust P, Roepstorff A, Wallentin M, Mouridsen K, Østergaard L (2006). It don’t mean a thing… Keeping the rhythm during polyrhythmic tension, activates language areas. Neuroimage, 31, 832-41.
I was asked what should we do instead of SHAM for a placebo. This approach is called efficacy study, comparing an experimental or active treatment to zero treatment. A more ethical approach when treating clinical populations is an effectiveness study, comparing the best conventional or popular protocol (or treatment, like Prozac, CBT) to the new experimental protocol, although not as rigorous.
Another approach is manipulating percent time in sham: For instance, GROUP A (Active) is 0% Sham, only active protocol 100% of time; GROUP B is 33% of the sessions SHAM, 67% Active, and GROUP C 67% SHAM, 33% Active. The percents could be sessions or blocks of time within a session
If sham training in fact is an active treatment, then its utility in an efficacy study is fatally compromised. I don’t see how using sham training in a graded fashion as you suggest is responsive to the basic problem here.
According to the Helsinki Declaration on the treatment of research participants, the use of placebo designs is regarded as unethical if an accepted treatment exists. The US is a signatory to this International agreement. This means that we should not be doing placebo-controlled studies of NF in application to ADHD in any event. But aside from it being unethical, it is also not very informative.
What we want to know is how it stacks up against the best available treatment, and in that regard we now have six studies that show it to be comparable in effectiveness to medication—in those areas where medication has its strongest effects.
Now once NF has been shown to be a valid active treatment, which actually happened some forty years ago, placebo designs are no longer relevant in the general case.
We have an active treatment. The question is, what can it accomplish for particular disorders?
We shouldn’t always have to start, with every disorder, with the project of ruling out the null hypothesis.