by Siegfried Othmer, PhD

I s it not remarkable that the entire field of education regards the challenges faced in education entirely without reference to the brain? This holds true from Arne Duncan at the Department of Education down to the local school board and even to the teacher in the classroom. It is almost as if the brain were not involved in the process. It is as if the neurosciences do not exist.
The fact that the technique Helen Irlen developed has not been universally adopted, even after proving itself for nearly thirty years of its existence, is testimony to this blinkered perspective. Here we have the combination of a simple evaluation tool and a simple remedy that could make a huge difference in the educational success of roughly 10 percent of students, a substantial fraction of those having difficulties.
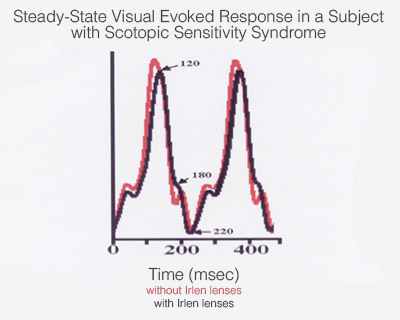
The theory underlying Irlen Syndrome now rests largely on a sophisticated study using magnetoencephalography in which it was shown explicitly, in a controlled design, that children afflicted with Irlen Syndrome differ in their visual processing capability from “normal,” and the use of the recommended remedy substantially restores appropriate visual processing capability.
This is about as “open-and-shut” as things get in research on brain function because we are still in the realm of sensory processing. The connection between this particular sensory processing issue and reading ability is by now also clear-cut. This is where data are by now plentiful that a child struggling to read can improve “instantly” by simply correcting for the visual processing deficit. This is accomplished by appropriately limiting the spectral input to the visual system. This requires nothing more complicated than eyeglasses that shape the spectral bandpass appropriately, according to the needs of the particular visual system.
What also appears to be the case is that brain function may be impacted more broadly, so that the affected children may also suffer from migraines, nausea, etc. This requires an additional hypothesis, namely that a localized disturbance in the brain can in fact disturb brain function more broadly. This is what we refer to in neurofeedback as the Disregulation Model. Effectively, the brain is burdened by having to come to terms with the challenge of visual processing, and this propagates throughout the brain.
It is not easy to frame the Disregulation Model in simple terms, but there is one central principle that can be easily stated. Since the focus here is on education, let me start with that topic. We have all observed in our own schooling that the brightest students didn’t actually study that hard, particularly in those subjects where understanding was challenged, such as the science and math courses, as opposed to those involved more in knowledge acquisition, such as history. The implication is that the really competent brain is actually not working very hard.
 Not only is this observation correct, it hints at a much larger truth. In actual fact, it is the learning disabled child who is working hard (along with being flogged to work even harder). This matches up with what is happening at the brain level. The competent brain is a brain at ease, whereas the learning disabled brain is struggling against internal resistances and interferences. This is a battle it will likely lose, which often manifests as an apparent lack of interest, possibly leading to eventual abandonment of the educational adventure entirely.
Not only is this observation correct, it hints at a much larger truth. In actual fact, it is the learning disabled child who is working hard (along with being flogged to work even harder). This matches up with what is happening at the brain level. The competent brain is a brain at ease, whereas the learning disabled brain is struggling against internal resistances and interferences. This is a battle it will likely lose, which often manifests as an apparent lack of interest, possibly leading to eventual abandonment of the educational adventure entirely.
Once we know this, our obligation is to minimize the interferences. It is largely pointless, as we know, to flog the learning disabled child to just “try harder,” “apply yourself,” etc. Neurofeedback is our method of choice to minimize the interferences to learning, and it does so marvelously. But neurofeedback training requires a substantial commitment of time and money. On a private-pay basis it cannot be made available to everyone.
If I now appraise the Irlen remedy from that same perspective, it looks like low-hanging fruit in the pursuit of educational competence. Certainly every child who comes to us for neurofeedback is given the support of Irlen lenses if that is called for. It eases the task of remediating their disregulation status and takes them to a more functional state.
We have even seen cases where brain training with neurofeedback has rendered the Irlen lenses superfluous. But these cases are not typical. And even in these cases, we cannot claim to have resolved the ultimate cause of the sensory processing deficit, which is a property of the eye that we cannot alter. Most likely, we have simply brought the brain to the point where it is no longer adversely affected.
On the basis of experience gained with Irlen lenses, neurofeedback, and auditory stimulation programs such as “The Listening Program,” most children who presently cannot keep up with educational demands will see their handicaps resolved. If not, then they may be helped further with programs such as Lindamood-Bell, Fast Forword, and others.
We would argue, however, that brain training such as neurofeedback and brain-based remedies such as Irlen lenses should come first, because we now know how to put the brain at ease so that it can learn. This is in accord with the latest neuroscience, which informs us that one key to the quality of brain function is the behavior of our resting state networks. That is what we are now training with infra-low frequency neurofeedback.
For a more in-depth review of Irlen Syndrome, see our earlier newsletter here: Scotopic Sensitivity Syndrome – An update