





Use of Infra-Low Frequency Neurofeedback in Trauma Recovery of Victims of Torture
by Siegfried Othmer | February 27th, 2017By Siegfried Othmer, PhD
Surely among the most intractable of conditions encountered in mental health practice are victims of torture. A number of these were among the war refugees being cared for in Sweden, and they have not responded to conventional therapies over a period of years in most cases. After good experience with trauma victims with Infra-Low Frequency Training in Malmö, Sweden a few years ago, the Swedish Red Cross decided to do a small pilot study with torture victims with treatment-resistance PTSD of long standing. Five such individuals were entered into the study, which was to involve twenty sessions of ILF neurofeedback.
The results were quite astounding. Summary trend data for all symptoms tracked are shown in Figure 1 for the five participants. If symptoms are further averaged over all five participants, the results of Figure 2 are obtained. Results are shown only for 18 sessions because the first data set was only acquired at the beginning of the second session, and the last set was acquired at the beginning of the 20th session. Nevertheless, global symptom severity showed a decline of more than 50% over these 18 sessions.
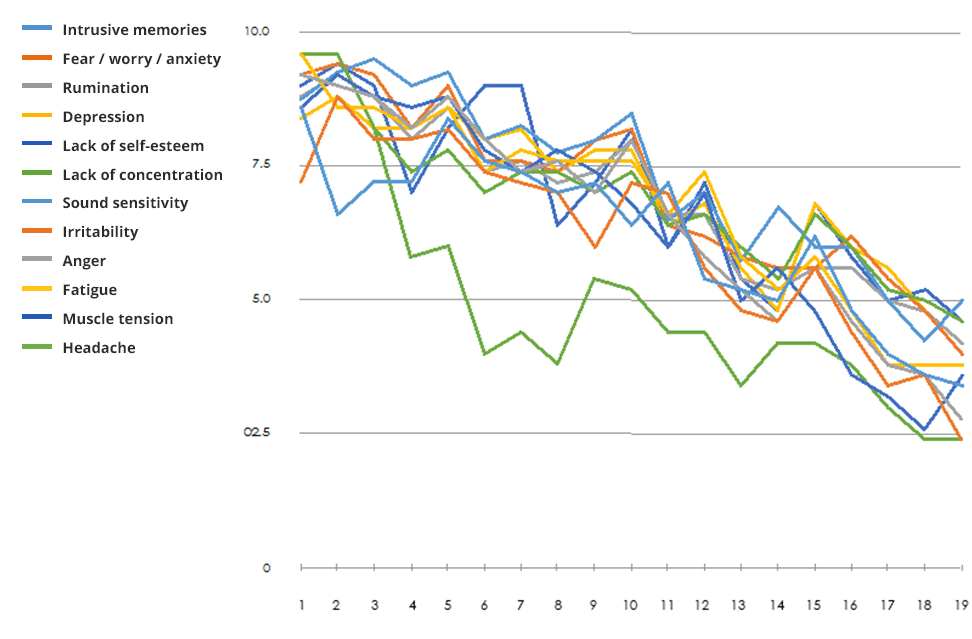
Figure 1: Average recovery curves for the five participants are indicated in the Figure for eighteen of the twenty sessions, for the symptoms listed in the legend. The first symptom appraisal took place only after the first session, and the last assessment took place at the twentieth session, and therefore does not reflect the gains attributable to the first and last sessions. Substantial remediation of their critical complaints is indicated.
When all the symptoms are averaged, the following curve is obtained:
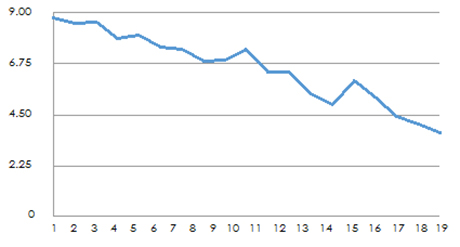
Figure 2: Average value for all patients and all symptoms. A decline by more than 50% in severity over the 18 sessions is observed.
The study was conducted under challenging real-life conditions. One participant received highly disturbing news about further violent death in the family back in her war-ravaged country, which made for setbacks in the training. A further handicap was that the clinicians supervising the sessions were themselves rather new to ILF neurofeedback, the method where clinical skills are particularly important because so much clinical decision-making is called for. ILF NF is self-executing in most respects, but not all! The technique is self-executing in the sense that the brain is very much in charge of what happens, but the clinician needs to know how to respond to the unfolding process for its most propitious outcome.
Not only is this population an inherent challenge to therapy, but victims of torture present a particular challenge to ILF neurofeedback. This is because one of the necessary counter-measures to physical torture is to disconnect from somatic signals from the body. This learned skill of dissociating from felt states then makes it more difficult to guide the ILF training appropriately. Moreover, when body signals are perceived, the tendency is to see them as alarm signals, which threatens to disrupt the calm state that is ideal for the training, and sometimes even catapult the client into states of extreme agitation. If one puts this together with the limited experience level of the clinicians involved, the impressive outcome is actually somewhat surprising.
There is no indication yet of a plateau being reached in the training, so additional sessions are likely to be useful. This is also expected on the basis of all the prior work with PTSD in general, and torture victims in particular, using the ILF method. The potential benefits have not been realized within twenty sessions. More likely, these five people are only at the beginning of a long process of recovery. After all, there are higher objectives to be achieved here than mere symptom abatement. These people are entitled to get their life back.
One other factor at work here is that the clinicians are all psychotherapists, and as such they see the neurofeedback mainly in a supportive role. As a result, there is a tendency to short-change the neurofeedback for the sake of getting clients back into psychotherapy as soon as they can handle it. Whereas it is clear that psychotherapy is needed here, it would be more efficient in our view to take the neurofeedback process to completion, including an opportunity for Alpha-Theta training, before emphasis is placed back on psychotherapy.
Siegfried Othmer, PhD
drothmer.com
—
Full Article:
Utilization of Infra-Low Frequency Neurofeedback in the Recovery from trauma of torture victims among war refugees in Sweden. (Unofficial translation. Not approved by the Swedish Red Cross)