A paper titled “A New Era of Precision Neuromodulation in Psychiatry” has just appeared in the journal JAMA Psychiatry, and it makes the case that precision neuromodulation is the new frontier in psychiatry (doi: 10.1001/jamapsychiatry.2026.1026). This remains within the tradition in medical psychiatry of working in deficit focus, albeit now with increasing technical refinement. The focus has shifted from locating deficits in nuclei such as the amygdala or the anterior cingulate (“hubopathies”), to localizing deficits in specific neural circuitry (“circuitopathies”).
With increasing clinical effectiveness comes a heightened sense of validation of the underlying model, understanding mental disorders as rooted in narrowly definable, localizable deficits. What has been missing is a systems-level perspective on neuro-regulation into which this would fit. In its absence, preoccupation has remained with the narrow tactical level rather than the globally strategic. A key barrier to progress along those lines has been the dualistic mind-body perspective that remains firmly entrenched as a practical reality, even as it has been superseded at the theoretical level. Psychiatry migrated from a psychodynamic focus that paid no attention to the brain to a medical model organized around discrete disorders that paid little attention to lived experience and was no longer interested in causal models.
What links psyche and soma is our regulatory regime, and yet psychiatry does not proceed from an understanding of how that system is organized and how it works. The over-arching, global perspective is missing. Looking at history, psychiatry has given us insulin shock, frontal lobotomy, and electro-convulsive shock therapy (which is still being done!). This reflects an adversarial posture, a willingness to bludgeon the brain into submission. We also have the catecholamine hypothesis, the neuromodulator deficit model. Its inadequacy makes the proffered remedy a case of ‘unilateral interference with nature.’ Presently, we have repetitive transcranial stimulation, delivered at levels just short of the generation of action potentials, much larger than necessary to the task of altering connectivity relationships. In sum, psychiatry has not shown respect for the brain. There is no recognition of the subtlety and complexity with which state regulation is organized.
The Diagnostic Statistical Manual ‘does not carve nature at its joints,’ in the colorful language of a Science Magazine editorial. The initiative to integrate physiological models into the DSM-V ran aground. The NIMH Research Domain Criteria failed to re-orient the field toward a systems-level perspective. Psychiatry has evolved into a conceptual cul-de-sac, albeit at a high technical level that within its own sphere can only inspire awe and command respect.
A Systems-Level Conception of our Neuro-Regulatory Regime
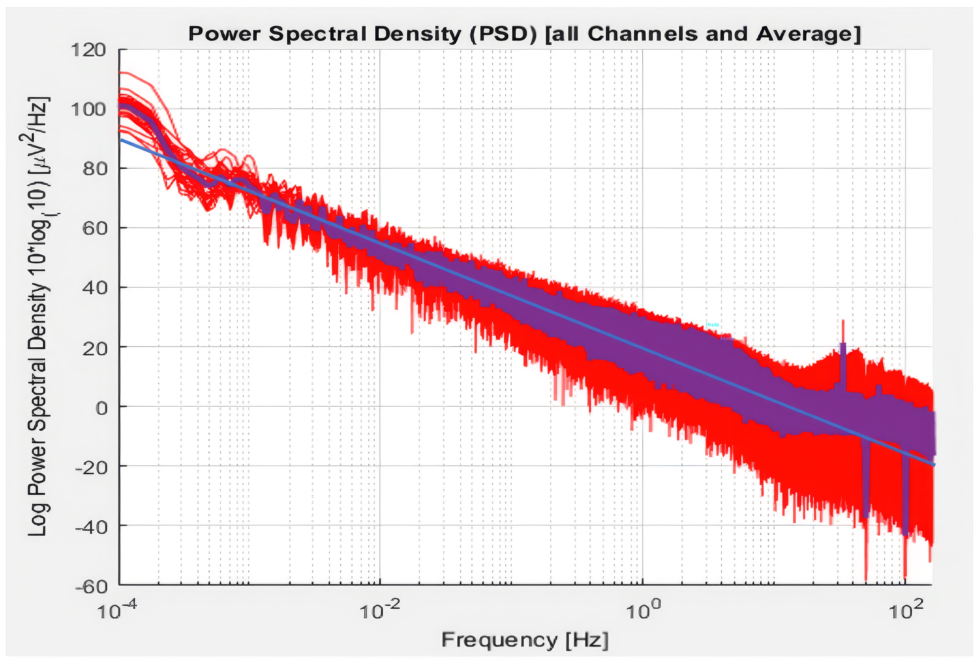
A systems-level perspective on neuroregulation might well proceed from the understanding that cerebral networks are hierarchically organized. Most likely, the most efficient point of appeal is then to the top of the regulatory hierarchy. For clinical purposes, advantage is taken of the fact that network function is organized according to frequency, which offers us our most discriminating and potentially most efficient access to network connectivity relationships and activation dynamics. With the frequency regime we arrive at a construct that is unitary, global in character, highly integrated, and exquisitely coordinated. The unitary character is illustrated in Figure 1. The spectral amplitude can be described with a single parameter over many orders of magnitude in frequency. We have hierarchical organization, with the lower frequencies establishing the context for higher ones. The functional hierarchy, the developmental hierarchy, the network hierarchy, and the frequency hierarchy jointly illuminate the self-regulatory genius of our brains.
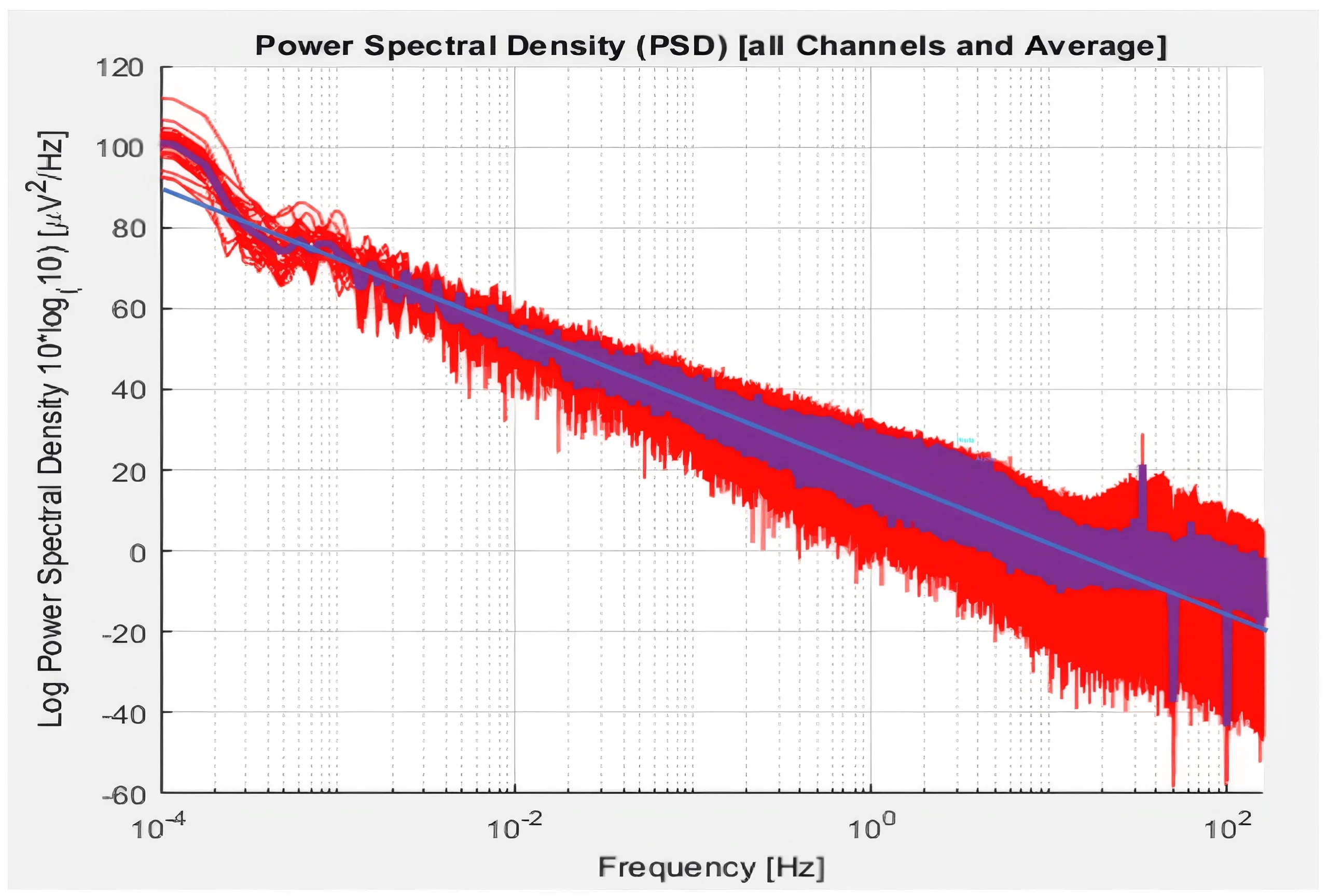
Figure 1. Spectral power (i.e., [voltage]2) is shown over six orders of magnitude in frequency for a 31-site montage. Individual channels are shown in red, and the average value is shown in purple. An eye-ball fit is shown in blue. A power-law relationship is indicated over the entire range. The power-law coefficient is 1.55. The deviation at higher EEG frequencies may be explained by extraneous factors such as muscle tension. (Data courtesy of Bee Medic, Switzerland.)
The brain must meet two contradictory requirements: it must be unconditionally stable, and it must be poised for rapid state change. Hence, it is organized to live at the edge of what is called ‘criticality.’ As this constitutes a key potential failure mode, the realm of brain dynamics becomes central to our concerns. Once we recognize the centrality of dynamic failure in mental health—the realm of cerebral instabilities and of their sub-clinical variants, of precipitous discontinuities in mental state—we find ourselves falling short with the stationary remedies such as psychopharmacology and fixed protocols in neuromodulation. At the level of subtlety, immediacy, and complexity with which good self-regulation must take place, assurance of stability cannot be outsourced to any technology.
A dynamical remedy is needed for problems in brain dynamics. While some mental disorders can be modeled as disorders of localized circuitry, our most intractable conditions tend to fall into the category of disorders of network stability. There is also a general principle at work here, namely, that the more dysregulated the system status, the greater the vulnerability to instability. We should therefore operate in the realm of temporal dynamics by which networks regulate themselves. Once we do that, we find that the approach works equally well for disorders where instability is not a paramount concern.
The Emergence of a Systems Perspective on the Frequency Regime
Clinical neurofeedback also progressed historically by way of a deficit focus, and of greatest relevance to our present challenge was the work with instabilities: seizures, migraines, and bipolar disorder. Working with seizure disorder, it was discovered that a simple protocol, SMR-training on the sensorimotor strip, was both calming and stabilizing. Working with migraines, the observation that lateralized training would drive the migraine to the other hemisphere led to a trial of inter-hemispheric placement at T3-T4. Thus constrained, the itinerant migraine vanished within minutes. If this tactic did not succeed at the standard beta1 band frequencies, it would likely still do so at a nearby frequency. This led to the discovery and exploration of the optimal response frequency (ORF) paradigm.
Working with Bipolar Disorder afforded even greater clarity. Training just above the optimal training frequency moves the brain in the direction of mania, whereas training just below takes the brain toward depression. These trends can become apparent in a matter of minutes. Fine adjustment of the training frequency allows us to find the balance point at which cerebral stability is likely achievable with additional training sessions.
Beyond migraines and Bipolar Disorder, the same approach generalized to other instabilities including seizures, panic disorder, asthmatic attacks, schizophrenia, trigeminal neuralgia, nocturnal myoclonus, restless leg syndrome, episodic suicidality, dysautonomia, dissociation, etc. A common failure mode is indicated. The relevant objective, by way of inter-hemispheric training at homotopic sites, is the subtle, dynamic coordination of the two hemispheres.
The special frequency is also optimal for other clinical conditions, so the principle generalizes. This implies that we have agency here. Requisite precision in the tuning of the target frequency may be at the one percent level in the EEG range. This implicates a resonance model. Exquisite sensitivity to even small shifts in frequency near the ORF confirmed it. This gave substance to the proposition that the ORF plays a generative, controlling role with respect to the frequency spectrum by way of a resonance mechanism.
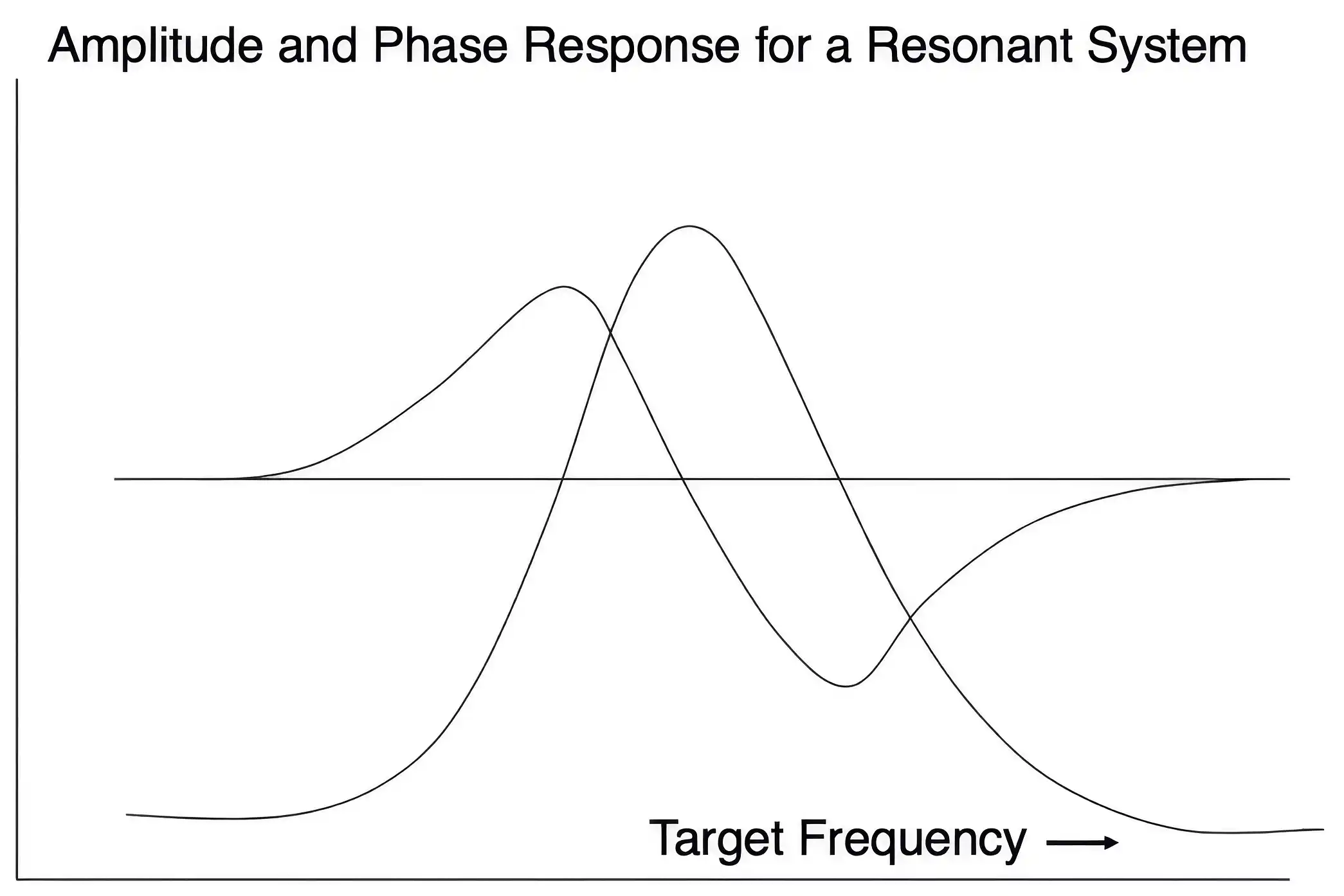
Figure 2. This graphic illustrates the universal resonance curve in its amplitude and phase response. Both become observable while fine-tuning the frequency in the vicinity of the ORF, thus lending support to the model. The system response differs qualitatively just above and below the ORF, which is expected based on the phase response characteristic. The peak in the amplitude distribution has been referred to as the “sweet spot” by trainees. It is experienced as a disambiguation of what transpires just above and below.
Empirically, we observe several optimal response frequencies distributed across the spectrum. These frequencies exhibit stable mathematical relationships among electrode placements. One set of relationships applies to the EEG spectral domain, whereas another set applies to the Infra-low frequency (ILF), Slow Cortical Potential domain. One set specifies the left-right relationship in lateralized protocols; another specifies inter-hemispheric placements. The relationship is non-harmonic in the EEG range, to secure non-interference. The relationship is harmonic in the ILF regime, to facilitate coordination. The two domains meet in the 2-4 Hz region of the Delta band. This is illustrated in Figure 3. Whereas ORFs individualize, the frequency rules generalize, and thus provide strong support for the model. The foundations of a systems-level conception of the frequency regime are now in place.
Figure 3. Frequency rules for lateralized training in the EEG and the ILF spectral regimes. In the EEG range, left-hemisphere training optimizes at 2 Hz higher than the right. In the ILF regime, training on the left optimizes at a factor of two higher than the right.
Clinical Approach
The clinical implications are both abundant and profound, in that exploitation of the ORF principle offers considerable potency when targeted directly in our training. The procedure is based on furnishing continuous information to the brain on its instantaneous state, as indexed by the time course of the signal—the narrow-band EEG or surface potential, derived from bipolar montage—at the ORF. There are no externalities here, so the brain readily internalizes the process, incorporating it into its regulatory schema. We have effectively furnished the brain with a “self-regulation prosthesis.”
The state shifts resulting from the feedback challenge typically become observable within minutes when we are dealing with dysregulated systems. The role of the skilled therapist is to adjust the parameter space to which the brain is exposed, in terms of target frequency and sensor placement, based on the state shifts and changes in symptom severity being observed within session, as well as client experience between sessions.
Over the course of 30 years, the training migrated episodically to ever lower target frequencies, eventually reaching the ultra-low range of micro-Hz—terra incognita in neuroscience. This is replicated, to a degree, in the course of a training. Upon selection of a starting frequency, the search for the ORF typically extends downward in frequency. The journey can cover several orders of magnitude. Empirically, we have found that training in the ultra-low frequency range yields the most encompassing clinical footprint with a minimum of drama. In the evolving model, the ultra-low frequency ORF constitutes the top of the frequency hierarchy. As such, it gives us the least ambiguous access to the homeostatic mechanism that organizes the realm of homeodynamics lying at higher frequencies. Core state regulation has been the primary objective all along. Precision neuromodulation was required to get there.
Meeting the Challenge of Trauma Formations
The most intractable conditions encountered in mental health are largely traceable to emotional and/or physical trauma in early childhood: Dissociative Identity Disorder, borderlines, and personality disorders in general. Also implicated are the major eating disorders, extreme obesity, extreme PMS, and chronic pain. Trauma is also a major compounding factor on other mental disorders. Early childhood trauma has been the principal driver to ever lower target frequencies, as we followed the imperatives of many brains to their most impactful ORF. The reason is now apparent: Complex trauma, neglect, and the emotionally absent mother profoundly distort the homeostatic and homeodynamic regime that gets shaped in the early years.
Insofar as the trauma response is situationally appropriate when kindled, recruiting response patterns that are latent in our physiology, the system resists its subsequent abatement. After all, if it was self-preserving many times in the past, it may be needed again. In the face of the challenge of early trauma, it became apparent that there is no higher priority than restoring homeodynamic competence to the nervous system, the essential first step in the path to recovery, a precondition for all other measures.
This shifts our orientation to the entirely positive and wholesome one of promoting core functional competence in the regulation of arousal, in the affective domain, in autonomic reactivity, as well as in interoception, the salience network. System stability remains the prime directive throughout. That affords us stability of state first and foremost, and it buttresses stability under challenge: allostasis. Once this agenda is accomplished, trauma therapies can proceed more productively, and other relatively intractable issues become more manageable—e.g., the problems of domestic violence, of addiction, and of criminality.
This brings us back, finally, to the dualistic divide in which our therapeutic disciplines are trapped. Trauma breaches the divide. Trauma syndromes cannot be resolved with exclusive reliance on psychiatry or psychodynamic psychotherapy. Bessel van der Kolk once said, with only modest exaggeration, that if one takes trauma out of the DSM, it would be reducible to a pamphlet. The pervasive impact of trauma on our physiology cannot be resolved merely by attending to what stands out in brain imaging.
Bessel also admonished trauma therapists: “Any therapy that does not put regulation front and center is likely to miss the mark.” EMDR and exposure therapy can readily trigger the further dysregulation of the client’s physiology. The promotion of core state regulation should therefore precede other interventions. We cannot erase trauma history. But with a full therapeutic palette, there is now a realistic prospect of access to an unencumbered life.
The full therapeutic palette must also include the Alpha-Theta experience, an EEG-prompted journey to a state of calmness that silences the verbal censor of our lives, thus facilitating an encounter with the core self. This occurs by way of imagery. The essential wholesomeness of the core self, despite everything that may have transpired, imbues the experience with a healing quality, and not rarely it is even transformational in character. The core self becomes an active agent in its own healing.
Endogenous Neuromodulation
The systems-level conception of our regulatory regime has led to several paradigm reversals: It has moved us from deficit-focused remedies to a function-focused approach. It has moved us away from prescriptive training to an adaptive process. In the words of Sue Othmer, “We are engaged in a dance with the brain, and the brain gets to lead.” It has moved us largely from event-based operant conditioning to continuous tracking of the optimal response frequency mechanism. Criticality of timing in the higher frequency range, combined with the subtlety of dynamics in the low-frequency range, advantages a scheme such as this in both the EEG and Infra-low frequency spectral regimes.
This more naturalistic feedback is appropriately referred to as Endogenous Neuromodulation. As an inherently dyadic process, combining first- and third-person perspectives on the brain’s response to a self-generated challenge, Endogenous Neuromodulation breaches the dualistic divide, portending a more organic approach to our most critical mental health challenges. With the addition of Alpha-Theta, we are recruiting both sides of the dualistic divide, the brain and the core self, as active agents in the healing journey. They engage us with their respective priorities.
“In order to alter nature, one must obey nature.”
“Problems are not necessarily solved at the level at which they appear.”
(Inspired by Albert Einstein)
Reference:
Endogenous Neuromodulation at Infra-Low Frequency: Method and Theory (2023)
Siegfried Othmer and Susan F. Othmer DOI: 10.20944/preprints202310.1085.v2
https://www.preprints.org/manuscript/202310.1085/v2